Abstract
Crusted scabies is an uncommon manifestation of parasitic infection caused by Sarcoptes scabiei var. hominis. This variant of scabies is seen in various immunocompromised states. Uncontrolled diabetes is an immunocompromised state which is characterized by increased incidence of various infections, and rarely, may be associated with this rare crusted scabies, which may pose a real diagnostic challenge. A high index of suspicion is required for timely and correct diagnosis in the best interest of the patient and the public health point of view to prevent the spread of this highly contagious infestation.
Keywords: Crusted scabies, Norwegian scabies, diabetes
Infections are more common in patients with diabetes mellitus in comparison to those without diabetes and course of the infections is also more complicated in this group of patients.1 Acquired defects in cellular innate and humoral immunity create an immunocompromised state and hence, incidence of more infections in uncontrolled diabetes.
Scabies is a skin disease caused by Sarcoptes scabiei var. hominis, an ectoparasite infestation, from family Sarcoptidae, class Arachnida, on the skin.2 A less common variant of it is known as crusted (Norwegian) scabies, which is a severe manifestation of this highly contagious skin infection. Crusted scabies has been described in patients with known immunocompromised states, like leprosy, immune deficiency disorders, human immunodeficiency virus (HIV) infection, organ transplant, chronic high-dose corticosteroid therapy, malnutrition, lymphoma, malignancy and also in elderly persons and those with Down’s syndrome and mental retardation.3 Diagnosis may be delayed and obscured in atypical clinical presentations that may resemble psoriasis, seborrheic dermatitits or even erythroderma in some cases.
Here we are reporting a case of crusted scabies in an elderly woman with neglected uncontrolled diabetes.
CASE REPORT
A 58-year-old female was admitted with uncontrolled diabetes and itchy skin lesions. She had a long-standing history of type 2 diabetes mellitus with hypertension of duration 20 years which was poorly controlled throughout this period. She was having itchy lesions over her trunk, face and extremities, which developed over the last 2 years. The eruption was gradual in onset and insidious in progression. Although the itching was intense and widespread, she had no itching on hands and feet, which may be due to peripheral neuropathy because of long-standing diabetes.
On clinical examination, the patient was moderately built, weighed 69 kg, height 152 cm with body mass index (BMI) - 29.86 kg/m2, blood pressure - 130/80 mmHg. On her dermatologic examination, there were widespread erythematous, hyperkeratotic/thickened plaques and excoriated areas on her trunk, face, scalp, ears and extremities. Intense hyperkeratosis with crusting and deep fissures were seen over elbows (Fig. 1A). Hyperkeratosis was also seen over hands with involvement of web spaces and wrist. Involvement of the nail plates was also seen with hyperpigmentation and cracking of the nail plates and subungual hyperkeratosis (Fig. 2A). Crusting was also seen over scalp, face and ears (Fig. 3A). Over the period of last 2 years, the patient had received multiple topical treatments in the form of steroids and antihistamines with poor response. None of the family members who reside with the patient complained of pruritus or any other symptoms.
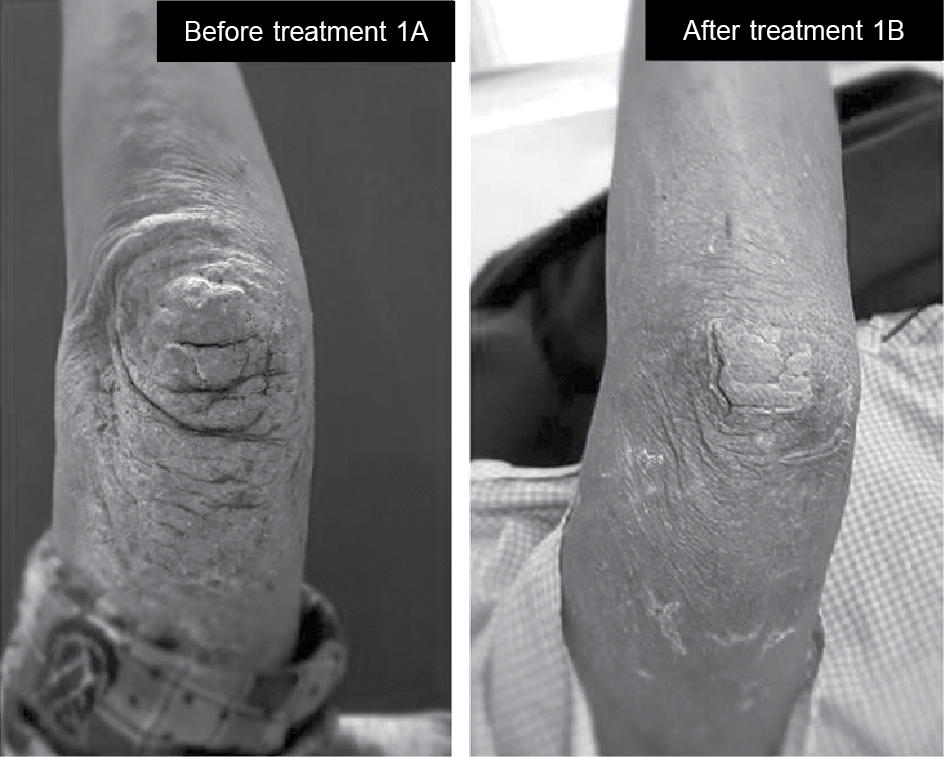
Figure 1A. Hyperkeratosis and deep fissures with excoriation over elbows. 1B Ten days after treatment, there was significant improvement in itching and skin lesions started resolving.

Figure 2A. Thick crusted hyperkeratotic lesion over hands and interdigital region. Involvement of nail plates with hyperpigmentation and cracking of nail beds. 2B. Same lesions with significant improvement 10 days after treatment.
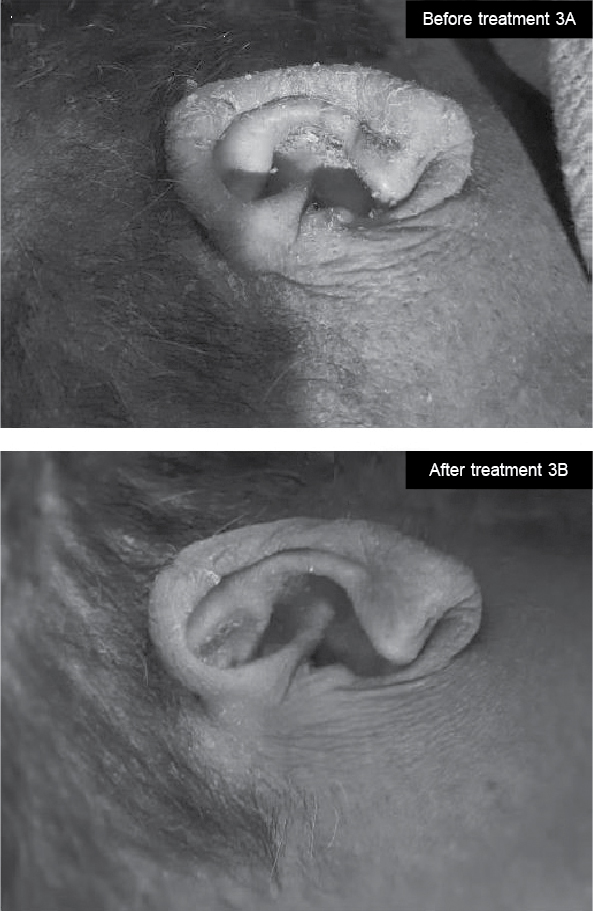
Figure 3A. Involvement of scalp and ear pinna with excoriated raw areas due to scratching of skin, which showed significant improvent after treatment (3B).
The laboratory examination revealed: White blood cells - 12,000 cells/mm3, platelet count - 1,28,000 cells/mm3, hemoglobin level - 7.8 g/dL, serum glutamic-oxaloacetic transaminase (SGOT) - 45 U/L, serum glutamic pyruvic transaminase (SGPT) - 38 U/L, serum creatinine - 0.6 mg/dL, fasting blood glucose - 180 mg/dL, postprandial glucose - 342 mg/dL. Her glycated hemoglobin (HbA1c) was 14.3%, thyroid-stimulating hormone (TSH) was 3.4 mIU/mL, total thyroxine (T4) was 8.6 µg/dL and vitamin B12 level was 458 ng/dL. HIV serology and other viral markers were nonreactive. Neurological examination with Semmes-Weinstein monofilament of 10 g showed a result of 0/6 in both feet. She had complete absence of temperature sensation, pin prick sensation and vibration perception with 128 Hz tuning fork which signifies complete loss of protective sensation (LOPS) in foot and severe peripheral neuropathy.
Differential diagnosis included psoriasis, severe seborrheic dermatitis and eczema. Due to the involvement of interdigital spaces and keeping in mind the long duration of disease unresponsive to topical or oral steroids, scabies was also kept as a differential diagnosis and scraping of the skin was taken from the lesions on the patient’s elbows and web spaces of the hands and nails. Scrapings were processed and prepared with 10% potassium hydroxide. On direct microscopic examination, a number of mites were seen (Fig. 4), hence confirming our diagnosis.
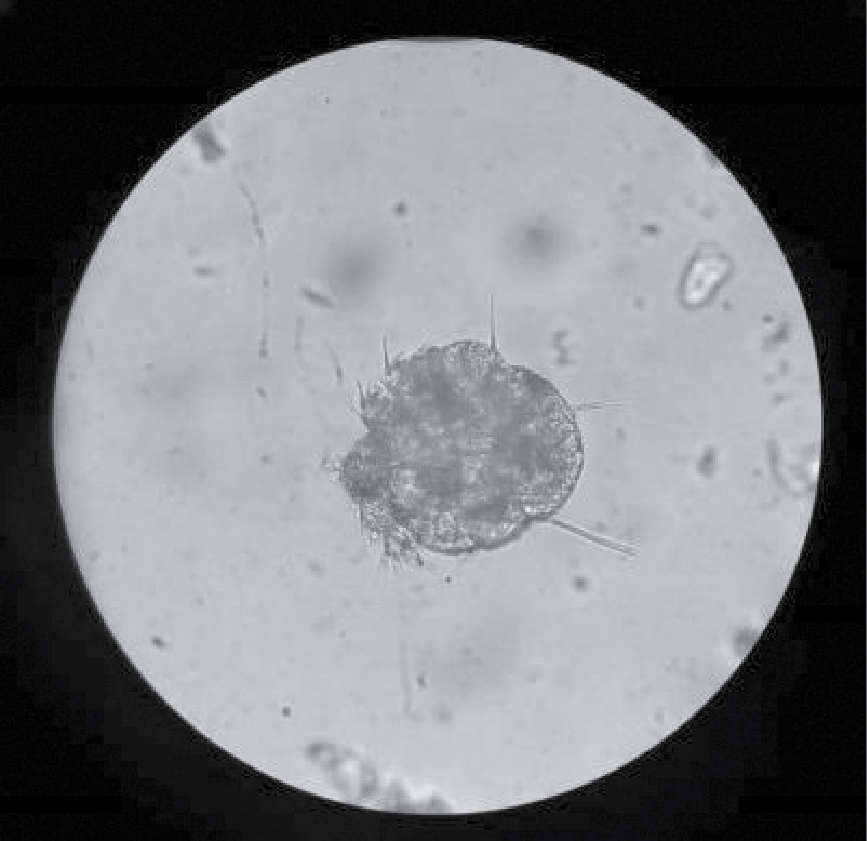
Figure 4. Mite of Sarcoptes scabiei from lesion scraping.
The patient was treated with topical 5% permethrin and oral ivermectin 12 mg. Permethrin 5% was given weekly for 3 weeks and ivermectin 12 mg was given on days 1, 2, 8, 9, 15 and 22.4-7 All the family members were treated with topical treatment with 5% permethrin weekly application for 3 weeks and were advised to thoroughly wash clothing and bedding with boiling hot water. Patient responded dramatically within a week of starting treatment with decrease in crusting and improvement in skin lesions and symptoms (Figs. 1B-3B).
DISCUSSION
Crusted scabies is a rare but severe manifestation of the common scabies, caused by the mite, S. scabiei var. hominis.2 Diagnosis of crusted scabies may be delayed owing to its variable, and in many cases, atypical presentation and lower incidence. Immunocompromised patients like those with leprosy, immune deficiency disorders, HIV infection, organ transplant, chronic high-dose corticosteroid therapy, malnutrition, etc., are at increased risk of developing crusted scabies infestation.3 Uncontrolled diabetes is a state of immuno-incompetency due to varied mechanisms. Decreased immunoresponse causes hyperinfestation and eventually severe manifestations of scabies.
An important cause of development of crusted scabies is failure of a surmountable immune response in body to suppress the proliferation of the parasite. Patients with a defective T-cell immune response or decreased cutaneous sensation, like in various neuropathies, may result in reduced ability to mechanically debride the mites by scratching, and hence, high parasite load. Hyperkeratosis of the skin, a prominent feature of crusted scabies, may be related to increased levels of cytokine interleukin-4.8 All the patients with this unusual presentation should be investigated for any underlying predisposing condition because immunocompetent individuals rarely develop crusted scabies.9
Itching is an important factor in the transport and transmission of parasites and destruction of burrows, which is usually absent in crusted scabies. Hence, the number of parasites may even exceed a million in crusted scabies and such patients are highly infectious.
In our patient, absence of itching in extremities may be due to peripheral neuropathy which is commonly found as a microvascular complication of long-standing diabetes mellitus and this may cause delayed detection and diagnosis of scabies.
The inflammatory response caused by heavy infestation may cause crusting and hyperkeratotic lesions. Though many clinical conditions like psoriasis, seborrheic dermatitis, dermatitis herpetiformis and chronic drug reactions may present with hyperkeratotic lesions of the skin, but in our patient, involvement of the web spaces with itching supported by the microscopic scrapings, nailed the diagnosis.
The treatment of crusted scabies is challenging because poor penetration of topical agents in hyperkeratotic skin and involvement of the nails and the high parasitic load may further complicate the clinical scenario. The patient must be isolated and the patient’s bedding and clothes must be disinfected. Nails are a frequent source of relapse, so they should be trimmed and proper application of scabicidal agent should be followed. A high index of suspicion is very important for timely diagnosis and treatment to avoid complications like impetigo, ecthyma or exfoliative dermatitis. In our patient, diabetes mellitus and associated neuropathy led to a delayed diagnosis of the condition, leading to unnecessarily prolonged misery for the patient.
We want to emphasize that the diagnosis of crusted scabies should be considered in resistant, long-standing, hyperkeratotic itchy skin lesions, in certain specific immunocompromised cases, and one of them is uncontrolled diabetes.
CONCLUSION
This case report signifies the importance of identifying crusted scabies with high suspicion in long-standing crusted hyperkeratotic lesions in a debilitated patient with immunocompromised status.
REFERENCES
- Deresinski S. Infections in the diabetic patient: strategies for the clinician. Infect Dis Rep. 1995;1:1-12.
- Burkhart CN, Burkhart CG. Scabies, other mites, and pediculosis. In: Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, WolffK (Eds.). Fitzpatrick’s Dermatology in General Medicine. 8th Edition, Vol 2. New York: McGraw-Hill; 2012. pp. 2569-77.
- Mehta V, Balachandran C, Monga P, Rao R, Rao L. Norwegian scabies presenting as erythroderma. Indian J Dermatol Venereol Leprol. 2009;75:609-10.
- Heukelback J, Feldmeier H. Scabies. Lancet. 2006;367:1767-774.
- Chosidow O. Clinical practices. Scabies. N Engl J Med. 2006;354(16):1718-27.
- Gunning K, Pippitt K, Kiraly B, Sayler LM. Pediculosis and scabies: a treatment update. Am Fam Physician. 2012;86(6):535-41.
- Huffam SE, Currie BJ. Ivermectin for Sarcoptes scabiei hyperinfestation. Int J Infect Dis. 1998;2(3):152-4.
- Walton SF, Beroukas D, Roberts-Thomson P, Currie BJ. New insights into disease pathogenesis in crusted (Norwegian) scabies: the skin immune response in crusted scabies. Br J Dermatol. 2008;158(6):1247-55.
- Costa JB, Rocha de Sousa VL, da Trindade Neto PB, Paulo Filho Tde A, Cabral VC, Pinheiro PM. Norwegian scabies mimicking rupioid psoriasis. An Bras Dermatol. 2012;87(6):910-3.