Abstract
Background: Coronavirus disease 2019 (COVID-19) pandemic has adversely affected the human health and wealth across the globe and is still posing a serious challenge to us. In the armamentarium of various drugs approved for COVID-19, remdesivir proved to be a major breakthrough in the treatment of moderate-to-severe cases. Our study is regarding its clinical efficacy and safety in hospitalized reverse transcription polymerase chain reaction (RT-PCR) confirmed adult patients with moderate-to-severe COVID-19 disease. Material and methods: A total of 100 patients with moderate-to-severe COVID-19 (RT-PCR positive) admitted in the intensive care unit (ICU) of Sri Krishna Medical College and Hospital (SKMCH), Muzaffarpur, Bihar, were enrolled in the study from 12th August to 11th November, 2020. All patients were given injection remdesivir as 200 mg IV loading dose on Day 1, followed by 100 mg IV daily for next 4 days along with other standard treatment. Results: Out of total 100 patients, 88 patients recovered and were discharged, while 12 patients died. Mean age of patients was 54 ± 16 years with male preponderance (4:1). Mean duration of hospital stay was 10.6 ± 5.4 days. C-reactive protein, D-dimer, ferritin and interleukin-6 decreased significantly after treatment with remdesivir, with p value <0.01, as compared to values at the time of admission, without any significant side effects. Conclusion: Early administration of remdesivir helps contribute to better clinical outcome in moderate-to-severe COVID-19 disease, without any significant side effects.
Keywords: Remdesivir, COVID-19, RT-PCR, morbidity, mortality, CT severity score, lab markers
Coronavirus disease (COVID-19) is caused by a coronavirus named severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2),1 which originated from Wuhan province of China. It soon spread across the globe and led to considerable damage to the healthcare system, economy and loss of human life. It is transmitted from symptomatic or asymptomatic persons through droplets or aerosols, and less commonly by direct contact of fomites.2 Despite global efforts and so many lockdowns, over 400 million people have got infected and over 5 million have succumbed to the disease, thus far.3
In view of its contagious nature, virulence, morbidity and mortality, various permutations and combinations of drugs came into the market, but none of them proved to be up to the mark.
In this connection, remdesivir got Food and Drug Administration (FDA) approval for emergency use on May 1, 20204 for the treatment of hospitalized patients with severe disease and on October 22, 2020, it was approved by FDA for use in adults and children aged >12 years weighing at least 40 kg for COVID-19 treatment requiring hospitalization.5 Remdesivir is a prodrug of an adenosine analog having broad-spectrum antiviral properties, including against coronaviruses, pneumoviruses, paramyxoviruses and filoviruses.
Previous studies indicate the benefits in terms of morbidity and mortality (11% vs. 15%), when remdesivir was used in hospitalized patients within 10 days of symptoms in moderate-to-severe COVID disease, as compared to placebo.6,7
MATERIAL AND METHODS
This study was conducted on 100 symptomatic reverse transcription polymerase chain reaction (RT-PCR)positive COVID patients admitted in intensive care unit (ICU) of Sri Krishna Medical College and Hospital (SKMCH), Muzaffarpur, Bihar from 12th August to 11th November, 2020. This was a prospective, observational, cross-sectional study based on data collected from patients.
- Inclusion criteria: RT-PCR positive, symptomatic, adult patients requiring ICU admission (oxygen saturation [SpO2] <94% on room air, high-resolution computed tomography [HRCT] thorax showing ground-glass opacities, raised inflammatory markers such as C-reactive protein [CRP], lactate dehydrogenase [LDH], ferritin, interleukin [IL]-6, D-dimer, etc.).
- Exclusion criteria: Age <18 years and >80 years, pregnant and lactating mothers, acute or chronic liver/kidney failure, malignancy.
Table 1 summarizes the demographic data of patients at admission.
|
Table 1. Demographic Data at Admission
|
|
Total number of patients (n)
|
100
|
|
Age (years)
|
54 ± 16
|
|
Sex
Male
Female
|
80
20
|
|
BMI (kg/m2)
|
23.8 ± 3.2
|
|
Blood pressure (mmHg)
SBP
DBP
|
118 ± 12
82 ± 8.0
|
|
Pulse rate
>100
60-100
<60
|
84
10
6
|
|
SpO2
>94%
<94%
|
30
70
|
|
Respiratory rate
<24
>24
|
34
64
|
|
Comorbidities
Diabetes mellitus
Hypertension
Coronary artery disease
COPD/Bronchial asthma
|
54
24
12
10
|
BMI = Body mass index; SBP = Systolic blood pressure; DBP = Diastolic blood pressure; SpO2 = Oxygen saturation; COPD = Chronic obstructive pulmonary disease.
A written informed consent was taken from all patients or their legal guardians. Intravenous remdesivir 200 mg was given as loading dose on Day 1, followed by 100 mg as maintenance dose for next 4 days, along with other standard treatments such as enoxaparin, methylprednisolone/dexamethasone, intravenous broad-spectrum antibiotics, etc., as per the Indian Council of Medical Research (ICMR) guidelines.
Outcome measures, in terms of clinical and biochemical improvement, duration of hospital stay, CT thorax changes, adverse effects, mortality, etc., were analyzed using Python 3 and Jupyter notebook. Continuous variables were expressed as mean ± SD (standard deviation). Statistical analysis was done for laboratory parameters at admission and at discharge using paired t-test, significance level being p < 0.05.
RESULTS
A total of 100 RT-PCR confirmed moderate-to-severely ill COVID-19 patients received remdesivir. The median age was 54 ± 16 years, with male preponderance (4:1). Fever (92%), breathlessness (90%), dry cough (78%), myalgia (56%), sore throat (46%) and loss of smell/ taste (11%) were the most common presenting clinical features (Table 2).
|
Table 2. Common Presenting Clinical Features
|
|
Clinical presentation
|
Percentage of patients
|
|
Fever
|
92
|
|
Shortness of breath
|
90
|
|
Dry cough
|
78
|
|
Myalgia
|
56
|
|
Sore throat
|
46
|
|
Loss of smell/taste
|
11
|
Associated comorbidities were diabetes mellitus (54%), hypertension (24%), coronary artery disease (12%) and chronic obstructive pulmonary disease (COPD)/bronchial asthma (10%) (Table 1).
Out of 100 patients, 22 patients did not need oxygen, 78 patients needed supplemental oxygen therapy. Oxygen was delivered through various modes, such as nasal prongs (5), face mask (18), nonrebreather mask (NRBM) (20), high-flow oxygen mask (18), noninvasive ventilation (NIV) (Bi-level positive airway pressure [BiPAP]) (12) and mechanical ventilation (5) (Fig. 1).
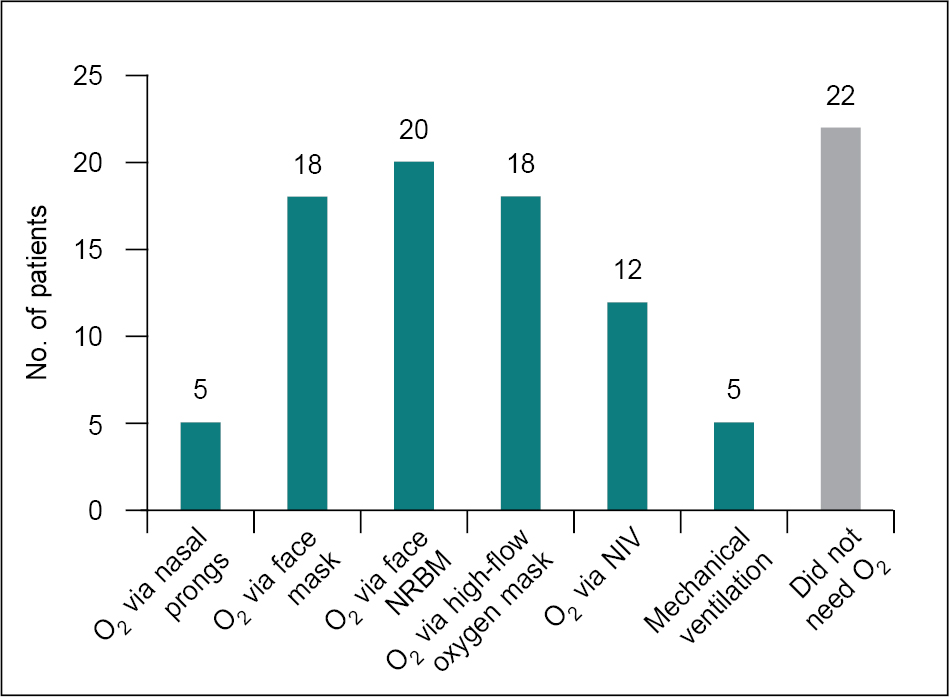
Figure 1. O2 requirement in patients (n = 100).
HRCT thorax was done on a 16 slice CT machine. Each of the five lobes were scored from 0 to 5. The mean CT severity score was 15 ± 5. The lung involvement pattern is depicted in Tables 3 and 4.
|
Table 3. Lung Involvement (n = 100)
|
|
% of lung involvement
|
No. of patients
|
|
<25
|
15
|
|
25-50
|
25
|
|
51-75
|
55
|
|
>75
|
5
|
|
Table 4. HRCT Pattern of Lung Involvement
|
|
Ground-glass opacity
|
100%
|
|
Consolidation
|
55
|
|
Bronchiectasis
|
11
|
|
Subpleural bands
|
13
|
|
Nodular opacities
|
2
|
Mean duration of hospital stay after remdesivir administration was 10.6 ± 5.4 days. There were no significant adverse effects. A total of 88 patients recovered and were discharged, while 12 patients died.
Considerable improvement in lab parameters was also noted after remdesivir administration, such as CRP, D-dimer, IL-6, serum ferritin, etc. (Table 5). The mean CT severity score in our study was 14.4 among improved and 18.2 among expired cases (Fig. 2).
|
Table 5. Inflammatory Markers (n = 100)
|
| |
Min
|
Max
|
|
CRP at admission (mg/dL)
|
8.4
|
137.6
|
|
CRP at discharge (mg/dL)
|
1.5
|
45.0
|
|
Ferritin at admission (ng/mL)
|
25.6
|
2436.0
|
|
Ferritin at discharge (ng/mL)
|
11.8
|
935.0
|
|
D-dimer at admission (µg/mL)
|
112.4
|
9582.0
|
|
D-dimer at discharge (µg/mL)
|
110
|
7225.0
|
|
IL-6 at admission (pg/mL)
|
2.4
|
1685.0
|
|
IL-6 at discharge (pg/mL)
|
2.0
|
175.0
|
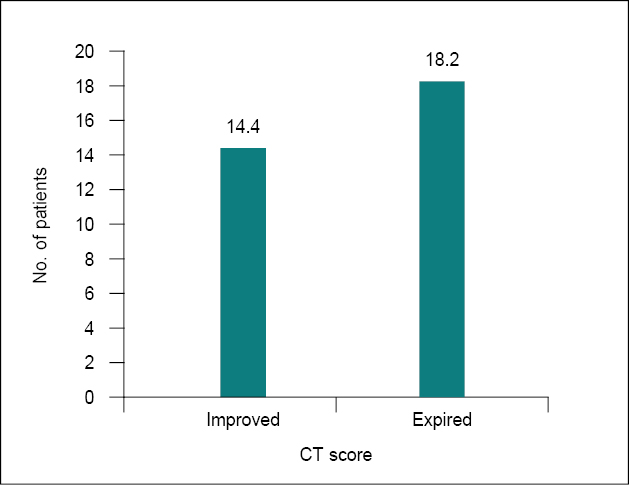
Figure 2. CT severity score.
DISCUSSION
Among the various treatment options available for COVID-19, remdesivir was the first drug to be approved for treatment by the US FDA.5 The efficacy of remdesivir in terms of hospital stay and associated mortality has been studied by several authors. Early administration of the drug resulted in better outcomes.
ACTT-1 study stated that remdesivir was superior to placebo in terms of hospital stay and better improvement in lower respiratory tract symptoms.8 Another study by Spinner et al stated clearly that 5 days of remdesivir was associated with higher odds of better clinical status distribution as compared with the standard treatment.9 Goldman et al demonstrated that there was no difference in clinical outcomes between a 5-day course and a 10-day course of remdesivir given to patients with severe COVID-19 not requiring mechanical ventilation.10
In our study, remdesivir was given to RT-PCR positive COVID-19 patients with moderate-to-severe disease, and its effect in terms of hospital stay and mortality (especially in those having comorbidities like diabetes mellitus, hypertension, etc.) was studied. It showed beneficial effects in terms of morbidity and mortality. In our study, mean duration of hospital stay after remdesivir administration was 10.6 ± 5.4 days, as compared to the study by Wang et al where the length of hospital stay in patients treated with remdesivir was 25 days.7
Our study has a limitation in the sense that it was not a case-control study.
CONCLUSION
From this study, we conclude that early use of remdesivir (within 5-8 days of symptom onset) in RT-PCR positive moderate-to-severe COVID-19 patients has a beneficial role in morbidity and mortality. It has positive impact on patient’s clinical as well as biochemical profile.
REFERENCES
- World Health Organization. Naming the coronavirus disease (COVID-19) and the virus that causes it. 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it
- Science Brief: SARS-CoV-2 and Surface (Fomite) Transmission for Indoor Community Environments. Available from: https://www.cdc.gov/coronavirus/2019-ncov/more/science-and-research/surface-transmission.html
- Available from: https://www.worldometers.info/coronavirus/. Accessed March 1, 2022.
- US FDA. FDA News Release - Coronavirus (COVID-19) update: FDA issues emergency use authorization for potential COVID-19 treatment. 2020. Available from: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-issues-emergency-use-authorization-potential-covid-19-treatment
- US FDA. FDA News Release: FDA approves first treatment for COVID-19. Oct 22, 2020. Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-covid-19
- Mehta RM, Bansal S, Bysani S, Kalpakam H. A shorter symptom onset to remdesivir treatment (SORT) interval is associated with a lower mortality in moderate-to-severe COVID-19: a real-world analysis. Int J Infect Dis. 2021;106:71-7.
- Wang Y, Zhang D, Du G, Du R, Zhao J, Jin Y, et al. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet. 2020;395(10236):1569-78.
- Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS, Kalil AC, et al; ACTT-1 Study Group Members. Remdesivir for the treatment of Covid-19 - Final report. N Engl J Med. 2020;383(19):1813-26.
- Spinner CD, Gottlieb RL, Criner GJ, Arribas López JR, Cattelan AM, Soriano Viladomiu A, et al; GS-US-540-5774 Investigators. Effect of remdesivir vs standard care on clinical status at 11 days in patients with moderate COVID-19: a randomized clinical trial. JAMA. 2020;324(11):1048-57.
- Goldman JD, Lye DCB, Hui DS, Marks KM, Bruno R, Montejano R, et al; GS-US-540-5773 Investigators. Remdesivir for 5 or 10 days in patients with severe Covid-19. N Engl J Med. 2020;383(19):1827-37.