Abstract
Postpartum hemorrhage (PPH) is a major cause of maternal morbidity and mortality. We focus on two innovations by Indian gynecologists, the Panicker’s vacuum suction cannula and the SR suction cannula. These effective devices are economical and easy-to-use, and help prevent and manage PPH. They can also be used to reduce bleeding in non-PPH indications. These Indian innovations are a matter of pride, and need to be studied extensively in diverse settings. This will help ensure that their benefits can be shared across the world.
Keywords: Atonic PPH, blood loss, India, LSCS, PPH, vaginal delivery
Postpartum hemorrhage (PPH) is a major cause of maternal morbidity and mortality.1 This is especially true in developing countries, where maternal health resources may be limited. Many of the known risk factors for PPH, such as prolonged labor, anemia and delayed operative intervention, are more common in such settings. The greatest risk is conferred by prior PPH due to any cause, placenta previa, placental abruption, uterine rupture and multiple gestation. Newer risk factors including hypertension, diabetes and ethnicity are also emerging.2
Even though there is significant interest in the diagnosis and treatment of PPH, current management strategies leave much to be desired. Uterine massage, oxytocin and methylergonovine are the standard of care, along with hemostatic drugs.3 In some cases, these do not prove sufficient hemostasis and invasive interventions such as internal iliac artery ligation and hysterectomy may be required. However, there is no concordance between various national guidelines4 and more effort is required to develop effective means of management.
IMPACT OF PPH
PPH is associated with a significant impact on maternal health, as well as on the healthcare system and healthcare costs.1 This impact worsens as the hemorrhage continues. It is rational, therefore, to develop means of preventing, limiting and managing PPH in a time-bound and cost-effective manner. Researchers across the world have proposed novel ways of diagnosing and stratifying PPH, as well as limiting it.5,6 Many of these methods and devices require technology, which is either inaccessible or unaffordable to persons working in resource-limited healthcare system. In such a situation, Indian innovations, the vacuum suction hemostatic devices, stand out as an efficient and extremely cost-effective method of preventing and managing PPH.
INNOVATION 1
Panicker7 proposed that creating negative pressure within the uterine cavity, using a cannula made of stainless steel or plastic, results in stoppage of bleeding from the postpartum uterus in women with atonic PPH and abnormal uterine bleeding (AUB). He inserted a 25 cm long cannula, 12 mm in diameter, with multiple holes of 4 mm diameter over the distal 10 cm of the cannula, into the uterus, through the vagina, to reach the fundus (Fig. 1). He connected the cannula to a suction apparatus to produce and maintain negative pressure of 700 mm mercury. This approach was tried in 55 women (40 post-normal vaginal deliveries and 15 post-lower segment cesarean sections [LSCS]) who experienced PPH refractory to uterotonic drugs used as standard of care.7
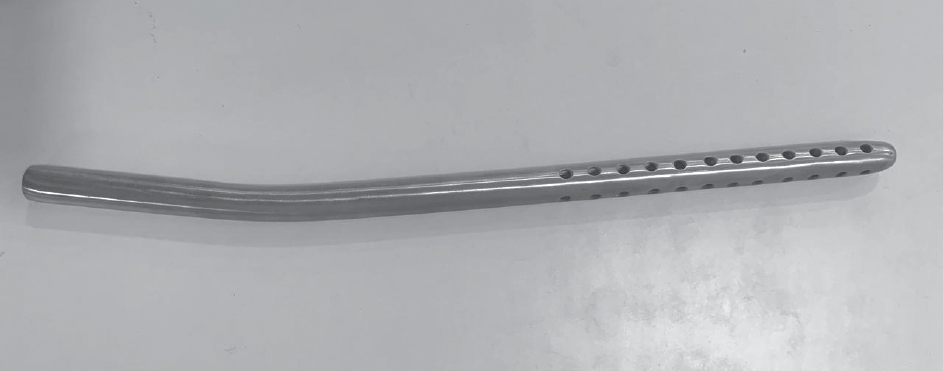
Figure 1.
Panicker reported his findings and highlighted the need to ensure accurate placement and care of the cannula, as well as to manage cervical and vaginal tears and lacerations concomitantly. The author also mentioned the limitations of the cannula, stating that it is effective only in managing uterine sources of bleeding. He suggested an improvisation in case a suction machine is not available, proposing the use of a mechanical suction unit of ventouse or manual vacuum aspiration (MVA) syringe.
INNOVATION 2
The Uterine Vacuum Retraction System, developed by HS Ram8 uses the SR suction cannula to control PPH after vaginal delivery. Vacuum retraction is created by negative pressure within the uterine cavity, using a cannula made of stainless steel, various lengths of cannulae are available (Fig. 2). The appropriate model, based upon size of uterus and mode of delivery, is inserted in the uterus, through the vagina, to reach the fundus. The cannula is connected to a suction apparatus to produce and maintain negative pressure of 650 mm mercury for 15 minutes.
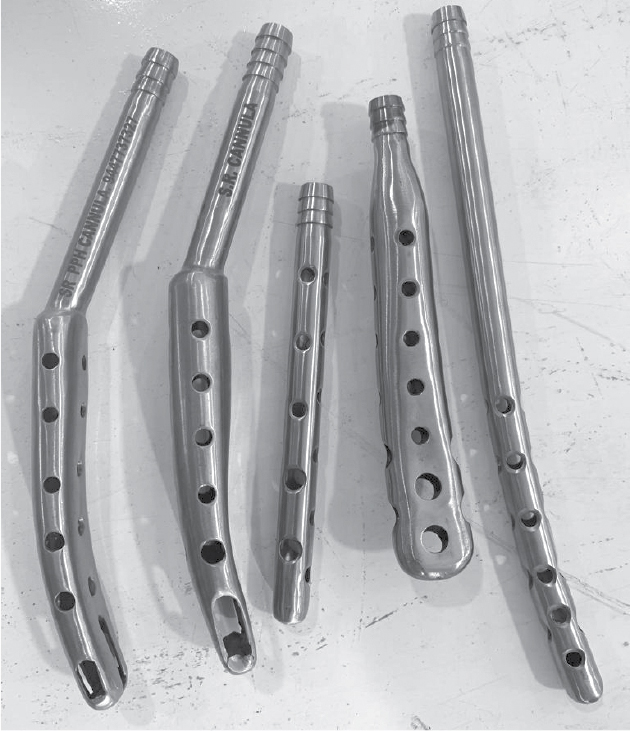
Figure 2.
The SR suction cannula was used to manage atonic PPH in an observational study. The bleeding stopped within 3 minutes in 60 women (50%); in 38 women (31.7%) bleeding cessation occurred between 3 to 4 minutes and in 22 women (18.3%) it took 4 minutes for the bleeding to stop. In 75 (62.5%) women, negative pressure was applied only once, in 20 (16.7%) it was applied twice, while in 25 women (20.8%) the negative pressure had to be applied three times to stop the bleeding. Blood collected in bottle after SR Cannula Application ranged from 100 to 150 mL.9
These innovations have been tried in multiple patients at our hospitals, and we attest to the efficacy and efficiency of these economical tools (personal experience).
INTROSPECTION
It is surprising; however, to see minimal research published on Paniker’s PPH cannula and SR vacuum suction cannula. Is this because these innovations are from resource-challenged medical care settings, and not from established “research” centers? Is it because these devices display their maximum benefit in peripheral centers, which do not have a “voice” in publications? Is it because the obstetricians who use these cannulae are so busy with their clinical work that they neglect publishing their data?
INSIGHT
Whatever the reason, we should celebrate Indian innovations with pride, rather than with prejudice.10 These innovative ideas deserve a fair chance, and must be studied in controlled settings, to assess their efficacy, safety and tolerability. The Indian vacuum devices are supported by experience and by eminence.
We suggest a pragmatic method of placing these devices in clinical practice (Table 1). The cannulae can be used for primary, secondary as well as tertiary prevention of atonic PPH, after both vaginal delivery and LSCS. Application of cannula helps clear the field of vaginal bleeding for better assessment and ease of stitching. As the cervical walls get apposed to the cannula, bleeding from cervical tear reduces and cervical stitching can be done in comfortable and clean environment.
|
Table 1. Usage of PPH Vacuum Suction Devices
|
|
Clinical usage
· Primary prevention: Prophylactic insertion when risk factors are present
· Secondary prevention: Insertion of device when excessive PPH is anticipated, e.g., rise in shock index
· Tertiary prevention: Curative insertion if bleeding is excessive
Caveats
· Check patency of cannula holes
· Check placement of tip of cannula at tip of fundus
· Check degree and duration of negative pressure
Check points
· Hemodynamic monitoring
· Local monitoring of cannula
Concerns
· Does not address cervical/vaginal bleed
· Does not obviate need for good obstetric and nursing care
|
We have used these devices in non-PPH indications as well. Small size cannulae can be used in endometrial polyp removal, scar ectopic and post-abortal heavy bleeding. Once backed by robust published evidence, these economical interventions will certainly find utility in maternity centers across the world, and serve to improve maternal health.
REFERENCES
- Bienstock JL, Eke AC, Hueppchen NA. Postpartum hemorrhage. N Engl J Med. 2021;384(17):1635-45.
- Ende HB, Lozada MJ, Chestnut DH, Osmundson SS, Walden RL, Shotwell MS, et al. Risk factors for atonic postpartum hemorrhage: a systematic review and meta-analysis. Obstet Gynecol. 2021;137(2):305-23.
- Feduniw S, Warzecha D, Szymusik I, Wielgos M. Epidemiology, prevention and management of early postpartum hemorrhage - A systematic review. Ginekol Pol. 2020;91(1):38-44.
- Dahlke JD, Mendez-Figueroa H, Maggio L, Hauspurg AK, Sperling JD, Chauhan SP, et al. Prevention and management of postpartum hemorrhage: a comparison of 4 national guidelines. Am J Obstet Gynecol. 2015;213(1):76.e1-76.e10.
- Zheutlin AB, Vieira L, Shewcraft RA, Li S, Wang Z, Schadt E, et al. A comprehensive digital phenotype for postpartum hemorrhage. J Am Med Inform Assoc. 2022;29(2):321-8.
- Wang D, Xu S, Qiu X, Zhu C, Li Z, Wang Z, et al. Early usage of Bakri postpartum balloon in the management of postpartum hemorrhage: a large prospective, observational multicenter clinical study in South China. J Perinat Med. 2018;46(6):649-56.
- Panicker TNV. Panicker’s vacuum suction haemostatic device for treating post-partum haemorrhage. J Obstet Gynaecol India. 2017;67(2):150-1.
- R. cannula application for atonic PPH during vaginal delivery. Available at: https://www.youtube.com/watch?v=pBReIEa3Ss4. Last accessed April 1, 2022.
- Damor P, Maheshwari S, Singh S. Role of SR vacuum cannula as novel technique for atonic PPH management study at Pannadhay Rajkiya Mahila Chikitsalaya and RNT Medical College, Udaipur. Int J Reprod Contracep Obstet Gynecol. 2021;10(11):4150-6.
- Ram HS. Comment on “Panicker’s vacuum suction hemostatic device for treating postpartum hemorrhage”. J Obstet Gynecol India. 2017;67(6):454-5.