Abstract
A perforated liver abscess mimics hollow viscus perforations. It may be accompanied by pneumoperitoneum and peritonitis. A hollow viscus perforation appears to be the most common cause of gas under diaphragm. In about 10% of the cases, it can be due to rare abdominal and extra-abdominal causes. One of the causes could be intra-abdominal infection caused by gas-forming organisms. We are reporting a rare case of pneumoperitoneum resulting from an unruptured liver abscess in an old male with no comorbidity. An unruptured pyogenic right lobe liver abscess in a 70-year-old male was accompanied by X-ray flat plate abdomen features suggestive of free gas under the right hemidiaphragm. Culture of the pus drained from liver abscess grew Klebsiella sensitive to piperacillin and tazobactam, and antibiotic treatment was administered.
Keywords: Liver abscess, gas under hemidiaphragm, intra-abdominal infection, gas-forming pyogenic liver abscess
Pyogenic liver abscess (PLA) is a key reason behind hospital admissions and life-threatening disease in low-middle income countries. Spontaneous gas-forming pyogenic liver abscess (GFPLA) is a rare nonsurgical cause of gas under right hemidiaphragm. The spectrum of GFPLA may mimic hollow viscus perforation because it is often associated with pneumoperitoneum and peritonitis. Escherichia coli and Klebsiella pneumoniae are among the most common pathogens causing pyogenic liver abscess.
In 85% to 90% of cases, pneumoperitoneum is due to perforation of a hollow viscus. In about 10% of the cases, it can be due to rare abdominal and extra-abdominal causes. One of the causes could be intra-abdominal infection caused by gas-forming organisms.
We report a rare case of pneumoperitoneum resulting from an unruptured liver abscess in an old male with no comorbidity.
CASE REPORT
A 70-year-old male, nonsmoker, nonalcoholic, presented with complaints of pain abdomen and fever for 15 days. He had history of open cholecystectomy 2 years back.
On examination, patient was febrile and abdominal tenderness was present over right hypochondrium; bowel sounds were present. His pulse rate was 110/min, blood pressure was 110/70 mmHg and respiratory rate was 20/min. Investigations done were as follows: Hemoglobin - 7.3 g/dL, total white blood cell count - 6900/cc, neutrophil - 50% and lymphocytes - 19.2%. His total bilirubin and direct bilirubin were normal. Serum glutamic oxaloacetic transaminase (SGOT), serum glutamic pyruvic transaminase (SGPT) and alkaline phosphatase (ALP) were increased around 10 times. His total protein and albumin were below normal. Chest X-ray and X-ray flat plate abdomen (FPA) in erect posture showed gas shadow under right hemidiaphragm (Figs. 1 and 2).
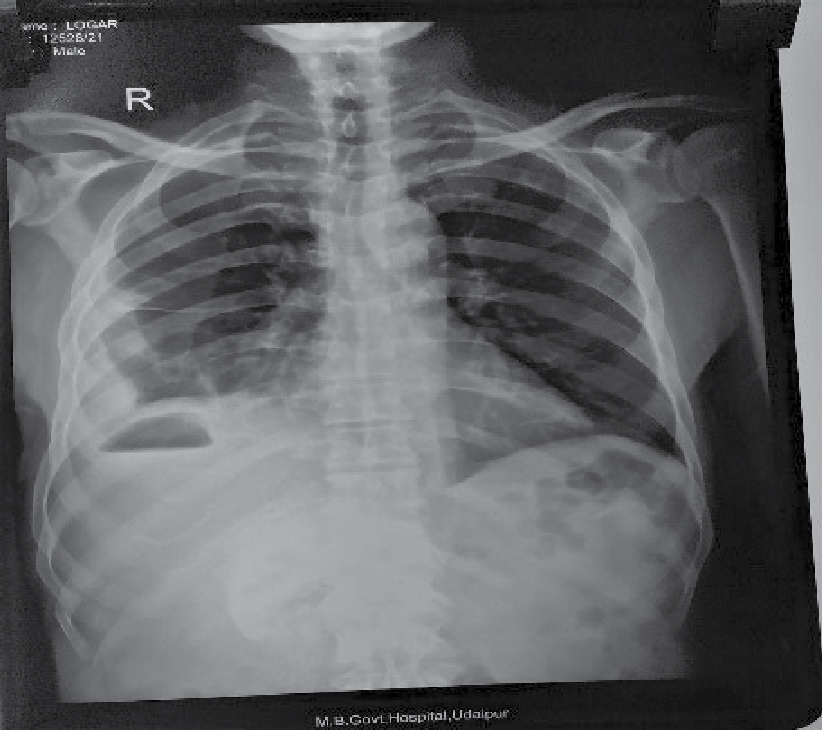
Figure 1. Chest X-ray PA view shows gas under right hemidiaphragm.

Figure 2. X-ray abdomen erect shows gas under right hemidiaphragm.
Abdominal ultrasound was done to look for possible cause of gas under right hemidiaphragm. Ultrasound abdomen showed moderate hepatomegaly with altered echotexture and abscess in right lobe of liver. After that, contrast-enhanced computed tomography (CECT) abdomen was performed which showed unruptured liver abscess as evident by intact capsule in right lobe and moderate hepatomegaly (Fig. 3 a and b).
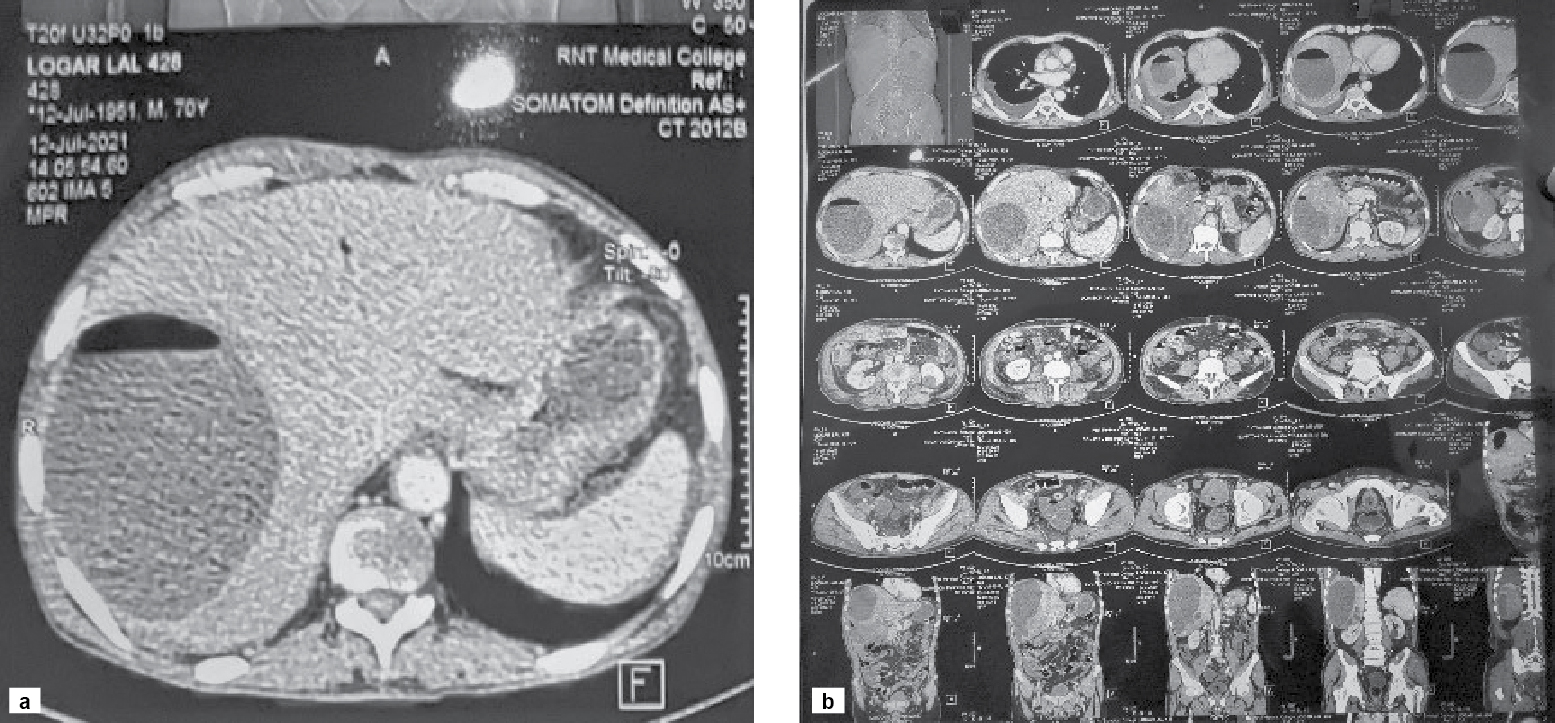
Figure 3 a and b. CECT abdomen shows a large well defined peripherally enhancing hypodense lesion with air fluid level in segment VII of right lobe of liver extending into segment VI also.
A clear air fluid level was visible on CT film inside the liver abscess. Liver abscess was drained (approximately 2 lt.) after confirmation of diagnosis. Pus was light yellow with greenish hue and was sent for culture and sensitivity which showed the growth of K. pneumoniae, sensitive to piperacillin and tazobactam. Treatment with antibiotic therapy was started.
DISCUSSION
Pyogenic liver abscess (PLA) is a pus filled pocket of fluid within the liver and it is a common infectious disease worldwide relating to a mortality rate ranging between 15% and 19%. GFPLA remains one of the most dangerous complications with a high fatality rate, in spite of aggressive management.
There are many possible causes of liver abscess, including diseases of the biliary system, a portal venous source arising from intestinal pathology, embolization of bacteria during hepatic surgery, abdominal infection, infection in blood, infection of the bile draining tubes and trauma that damage the liver, but in 15% to 45% of cases, it is cryptogenic where no cause is identifiable. Most are single and insidious in onset, as the case reported here. In approximately 40% of cases, hepatic abscesses are polymicrobial. Anaerobic organisms are involved in approximately 40% to 60% of the cultures, the most common organisms being E. coli and K. pneumoniae.
In this particular case, the patient showed signs and symptoms of acute abdomen and radiological evidence of gas under right hemidiaphragm. A provisional diagnosis of gastrointestinal perforation was made. Bowel perforation and recent surgical procedure are commonest causes of pneumoperitoneum.
The chest X-ray and X-ray FPA are abnormal in approximately 50% of the cases, with findings reflecting subdiaphragmatic pathology, such as an elevated right hemidiaphragm, right pleural effusion or atelectasis. Occasionally, there may be left-sided findings in the case of an abscess in the left lobe of the liver.
Pneumoperitoneum is a rare radiological finding in liver abscess. It usually results from the perforation of an intraperitoneal hollow organ, in which case, it is considered a surgical emergency (in 85% to 90% of cases). Only about 10% of pneumoperitoneum cases have nonsurgical causes, for which surgical intervention is usually not required.
In this case, liver abscess filled with pus and having air fluid level visible in CECT abdomen, was responsible for gas under right dome of diaphragm in chest X-ray and X-ray FPA in erect posture.
CONCLUSION
Liver abscess with intact capsule, having air fluid level, imparting the radiological finding of gas under right dome of diaphragm on X-ray FPA in erect posture, is a rare nonsurgical finding. Every case of pneumoperitoneum is not due to a perforated hollow viscus. In this case, the air fluid level inside the cavity of liver abscess was attributed to the gas-forming organism K. pneumoniae.
SUGGESTED READING
- Kumar N. Ruptured liver abscess presenting as pneumoperitoneum. Hellenic J Surg. 2017;89(3-4):172-4.
- Pham Van T, Vu Ngoc S, Nguyen Hoang NA, Hoang Huu D, Dinh Duong TA. Ruptured liver abscess presenting as pneumoperitoneum caused by Klebsiella pneumoniae: a case report. BMC Surg. 2020;20(1):228.
- Khim G, Em S, Mo S, Townell N. Liver abscess: diagnostic and management issues found in the low resource setting. Br Med Bull. 2019;132(1):45-52.
- Qian Y, Wong CC, Lai S, Chen H, He X, Sun L, et al. A retrospective study of pyogenic liver abscess focusing on Klebsiella pneumoniae as a primary pathogen in China from 1994 to 2015. Sci Rep. 2016;6:38587.
- Sabiston Textbook of Surgery. 21st Edition, Chapter 54; pp. 1452-53.