Abstract
Coronary artery anomalies are rare, and the incidence is around 1 to 2% in the general population. Majority of the patients are asymptomatic and detected while investigating another clinical issue. A few anomalies may be life-threatening due to the malignant course with potential for ischemia and even sudden death. Multidetector computed tomography (MDCT) has high accuracy in detecting these anomalies because of volume rendering (VR) and multiplanar reconstruction (MPR). ‘High take-off’, origin of the coronary artery from the opposite or noncoronary cusp with anomalous course and coronary artery fistula are three most frequent anomalies. MDCT can be a useful screening tool in the study of coronary anomalies.
Keywords: Coronary artery anomalies, MDCT, high take-off
Coronary artery anomalies are rare, and the incidence is around 1% to 2% in the general population. Multidetector computed tomography (MDCT) has high accuracy in detecting these anomalies because of volume rendering (VR) and multiplanar reconstructions (MPRs). Majority of the patients are asymptomatic and detected while investigating another clinical issue. A few anomalies may be life-threatening due to the malignant course with potential for ischemia and even sudden death. Moreover, failure to cannulate these vessels during conventional angiography can be minimized if the existence of these anomalies is known to the operator. This article presents an unpublished retrospective case series and review of literature of common coronary anomalies detected on MDCT.
At Nizam’s Institute of Medical Sciences (NIMS), Hyderabad, 770 patients underwent CT-conventional coronary angiography (CAG), on 128-slice single source MDCT (SOMATOM Definition AS ± SEIMENS) during the last 3 years (unpublished data). On analysis, coronary artery anomalies were found in 23 patients (3%). Their ages ranged from 25 to 82 years. Majority of the cases were in 51 to 60 years age group. Among them, 17 were males. The most common anomaly seen was high take-off of coronary arteries, seen in 10 cases. Of them, 2 were having high origin of right coronary artery (RCA) (Fig. 1), 7 were having high origin of left main coronary artery (LMCA) and one was having high origin of both coronary arteries with acute kink at the origin of RCA. Anomalous origin of coronary artery from opposite sinus was seen in 8 cases (Figs. 2-5). RCA from left coronary sinus with interarterial course between aorta and right ventricular outflow tract was seen in 5 cases. Anomalous origin of left coronary artery (LCA) from right coronary sinus with interarterial course between aorta and right ventricular outflow tract was seen in 2 cases. Anomalous origin of left circumflex artery (LCx) from right coronary sinus with retroaortic course was seen in 1 case (Fig. 6). Separate ostia for left anterior descending artery (LAD) and LCx was noted in 3 patients (Figs. 7 and 8). Shepherd crook deformity of proximal segment of RCA was seen in 1 patient. Super-dominant RCA with absent LCx was seen in 1 patient (Fig. 9).
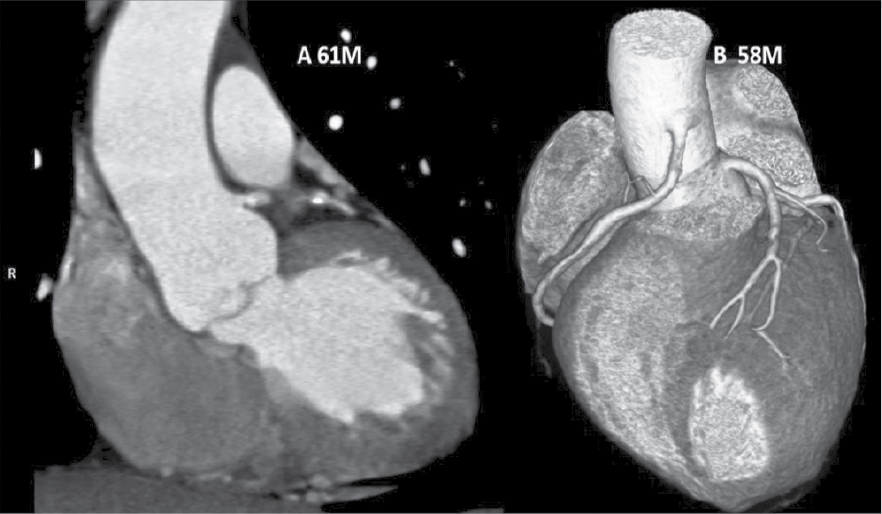
Figure 1. Two different patients of ‘high take-off’ of LCA in patient aged 61/M and RCA in patient aged 58/M.
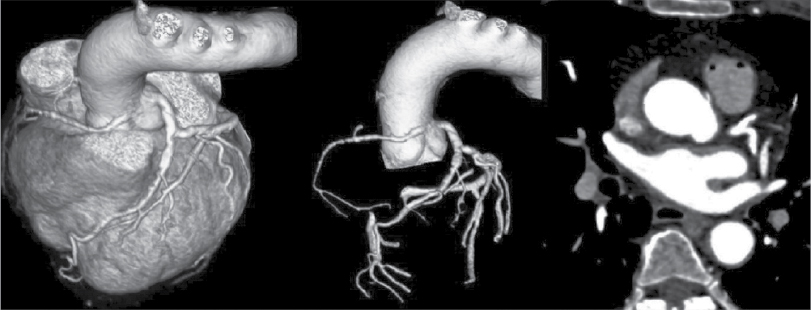
Figure 2. VRT and axial images of a patient (55/F) showing RCA originating from left coronary sinus of Valsalva. Course of RCA is interarterial.
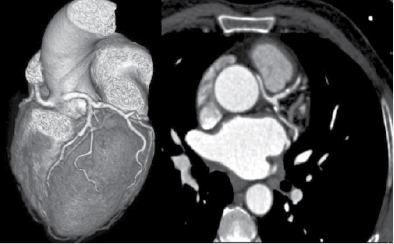
Figure 3. VRT and axial images of a patient aged 59/M depicting the origin of LCA from RCA having interarterial course.
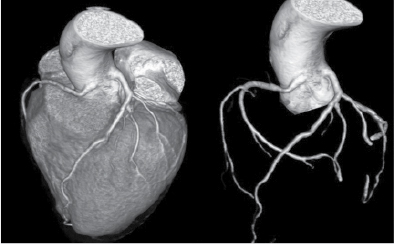
Figure 4. Origin of RCA and LCA from left coronary sinus in a patient aged 35/M.
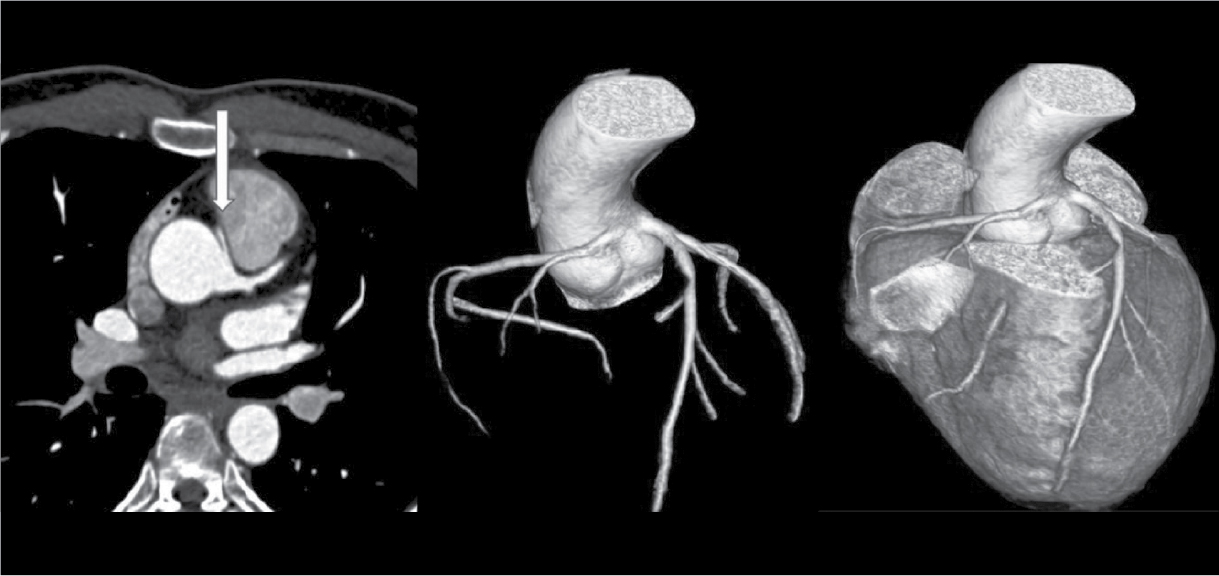
Figure 5. Origin of RCA and LCA from left sinus of Valsalva with interarterial course of RCA in a patient aged 25/M.
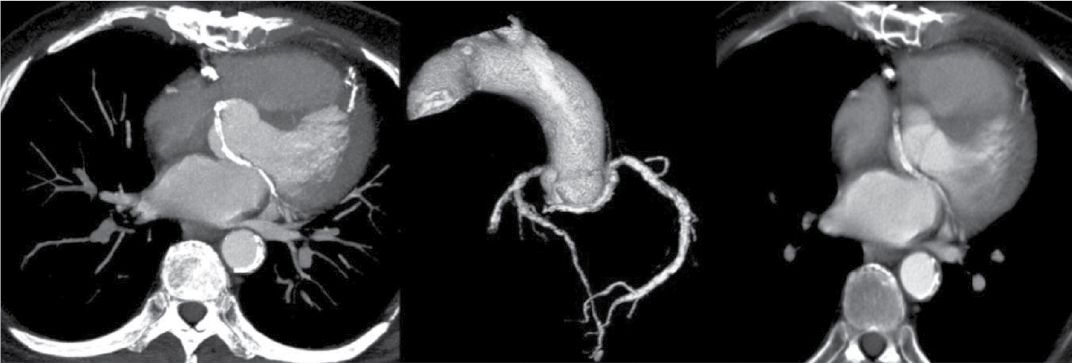
Figure 6. LCx is originating from right coronary sinus with retroaortic course in axial and VRT images of patient aged 82/M.

Figure 7. Two patients aged 48/M and 57/M, CT-CAG VRT images showing separate origin of LAD, LCx and there is no LMCA.

Figure 8. Separate origin of LAD and LCx in a patient aged 71/M.

Figure 9. A patient aged 52/F having super-dominant RCA. LCx is absent.
The prevalence of coronary anomalies is reported to be approximately 0.3 to 1% in various studies.1 Due to lack of uniformity of diagnostic criteria, the true incidence is not known. Any coronary pattern with deviation in the number of ostia, variation in the sinus of origin, the course that is not common in the general population, can be counted as an anomaly. It is important to categorize them as major or minor depending on their potential for clinical consequence. With advances in noninvasive imaging, more anomalies are getting diagnosed compared to autopsies or invasive cine-angiograms. Recent advances in MDCT technology with 100% sensitivity in detecting these anomalies, have made it a more acceptable diagnostic tool. Although majority of the anomalies are benign with conceptual and educational interest, a few have potential for ischemic symptoms, and even sudden cardiac death especially during exercise or during competitive sports. The anomalies associated with structurally abnormal hearts have to be a special group due to their importance during the surgical correction. It is most convenient to consider the isolated coronary anomalies as − 1) Anomalies of the origin and course (High origin, ostia in unexpected sinus, single coronary artery, separate LAD and LCx, etc.); 2) Anomalies of the intrinsic anatomy (Coronary ectasia, hypoplasia, total absence, etc.); and 3) Anomalies of termination (Coronary-cameral fistulae, etc.).
The authors observed coronary anomalies in 3% that is 23 out of 770 cases using 124 slice MDCT. In a study, 6,014 consecutive patients that underwent 64 slice MDCT were analyzed by Yang et al and coronary anomalies were found in 66 (1.09%) patients. All had one or more symptoms like chest pain, dyspnea, palpitations, arrhythmias and myocardial infarction. They found high take-off, origin of the coronary artery from the opposite or noncoronary cusp with anomalous course, and coronary artery fistula as three most frequent anomalies. They opined that due to VR technique in CT angiograms they identified a few lesions, which were not clear in conventional cineangiograms.2
Most common anomalies are high origin of coronaries from aorta with a normal course. There are cases when RCA arises few millimeters above sinotubular junction, but distance of 2 cm has also been recorded.3 In our experience, there were 10 (1.3%) out of 770 cases with high take-offs. High take-off usually has no clinical problems but may cause difficult cannulation. Incidence is 0.60% as per a study by Fujimoto et al in their series of 5,869 cases.4
Multiple ostia of right and left coronaries can be considered as important anomalies. RCA and conus branch may arise separately. Similarly, LAD and circumflex arise separately with no LCA, which accounts for small percentage with normal course. Incidence of separate ostia for LAD and LCx from left coronary sinus was 0.26% in a series.4 In our series, we had 3 cases of separate origin of LAD and LCx accounting for 0.39%.
Origin of coronary artery or branch from the opposite or noncoronary sinus is another anomaly that is commonly observed. These anomalies are classified into 4 types. One is interarterial course between aorta and pulmonary artery. Second one is retroaortic course. Third is prepulmonic and septal or subpulmonic course. The interarterial course is clinically important as it is associated with sudden death.5 Fujimoto et al, in their series of 5,869 cases, noted that 29 cases had opposite coronary sinus and in 27 of these cases RCA arose from left coronary sinus.4 All these cases had interarterial course. It is reported that 30% of these have sudden cardiac death. Anomalous origin of coronary artery from opposite sinus was seen in 8 cases accounting for 1.04%. RCA from left sinus were 5 and LCA from right coronary sinus were 2 with interarterial course. In 1 case, LCx was arising from right coronary sinus with retroaortic course.
Finocchiaro et al in their study of 5,100 cases found anomalous coronary arteries in 0.6%. Anomalous left coronary artery (ALCA) arising from right sinus of Valsalva with interarterial course (11) and RCA originating from left sinus of Valsalva (RACA) with interarterial course (11) were most commonly found. ALCA arising from pulmonary artery was present in 7 cases and in 1 case, the LCA arose from noncoronary sinus.6 In a similar study by Nguyen, the incidence of anomalies was 47 out of 9,572 cases (0.49%). LCx from RCA/right sinus of Valsalva was seen in 31.9%. High take-off of RCA was seen in 23.4%, RCA from left coronary sinus was noted in 17% and LCA from right coronary sinus was seen in 10.6%.7 Approximately 1.04% of our cases had anomalous origin of coronary artery (5 RCA and 2 LCA, and in 1 LCx was originating from right coronary sinus with retroaortic course).
Super-dominant RCA with absent LCx artery is an exceedingly rare congenital anomaly that can be confused with atherosclerotic total occlusion. There are a few such case reports in the literature.8 We observed one such case of super-dominant RCA with absent LCx. Single coronary artery is extremely rare with prevalence of 0.09% (5 out of 5,869 cases) in a study by Fujimoto et al.4 Its clinical implication is complex when the patient develops atherosclerosis in the proximal segment and it can be a challenging situation for either angioplasty or coronary artery bypass grafting (CABG).
CONCLUSION
Due to the noninvasive nature of the modality and the advantage of VR and MPR techniques, MDCT can be a useful and preferred screening tool in the study of coronary anomalies.
REFERENCES
- Angelini P, Velasco JA, Flamm S. Coronary anomalies: incidence, pathophysiology, and clinical relevance. Circulation. 2002;105(20):2449-54.
- Yang S, Zeng MS, Zhang ZY, Ling ZQ, Ma JY, Chen G. Sixty-four-multi-detector computed tomography diagnosis of coronary artery anomalies in 66 patients. Chin Med J (Engl). 2010;123(7):838-42.
- Thakur R, Dwivedi SK, Puri VK. Unusual “high take off” of the right coronary artery from the ascending aorta. Int J Cardiol. 1990;26(3):369-71.
- Fujimoto S, Kondo T, Orihara T, Sugiyama J, Kondo M, Kodama T, et al. Prevalence of anomalies origin of coronary artery detected by multi-detector computed tomography at one center. J Cardiol. 2011:57(1):69-76.
- Roberts WC, Siegel RJ, Zipes DP. Origin of the right coronary artery from the left sinus of valsalva and its functional consequences: analysis of 10 necropsy patients. Am J Cardiol. 1982;49(4):863-8.
- Finocchiaro G, Behr ER, Tanzarella G, Papadakis M, Malhotra A, Dhutia H, et al. Anomalous coronary artery origin and sudden cardiac death: clinical and pathological insights from a National Pathology Registry. JACC Clin Electrophysiol. 2019;5(4):516-52.
- Nguyen VT. MDCT in diagnosis of anomalies of coronary artery origin and course: a coronary MDCT-Angiographic study of 9572 patients. Vascul Dis Ther. 2019;4:1-7.
- Shaikh SSA, Deshmukh V, Patil V, Khan Z, Singla R, Bansal NO. Congenital absence of the left circumflex artery with super-dominant right coronary artery: extremely rare coronary anomaly. Cardiol Res. 2018;9(4):264-7.