Abstract
Injuries due to a lightning strike are uncommon presentations in the emergency department. Common injuries caused by lightning include burns, muscle pains, cardiac arrest, hearing loss, seizures, behavioral changes and ocular cataracts. We report a case of a 26-year-old primigravida with history of 3 months of amenorrhea who was struck by lightning as she was standing beside a tree. It left her unconscious, immediately after which she was taken to the emergency department of Maharana Bhupal Govt Hospital (MBGH Hospital), Udaipur, Rajasthan. Entry wound was from right ear and the exit wound was on abdomen. Examination confirmed linear first- and superficial second-degree burns. The electrocardiogram (ECG) showed deep and symmetrical T-wave inversion in precordial and lateral leads. There was an associated elevation of troponin T levels (peak: 432 ng/L), suggestive of myocarditis. On otoscopic examination, she was found to have rupture of tympanic membrane bilaterally. A transthoracic echocardiography revealed reduced ejection fraction of the left ventricle to 25% with global left ventricle hypokinesia, moderate mitral regurgitation and tricuspid regurgitation. This case aims to raise awareness among the healthcare providers regarding multiple organ involvement in lightning injury.
Keywords: Lightning, seizures, myocarditis, echocardiography
Lightning injuries are injuries caused by a lightning strike. An interdisciplinary approach towards patients with muti-organ injuries following lightning strike is significant. Lightning strike is a common cause of sudden cardiac death and is also associated with injuries to several organ systems.1,2 Lightning injuries are divided into direct strikes, side splash, contact injury and ground current.3
Presented here is the case of a 26-year-old woman who was struck by lightning and developed multi-organ injuries.
CASE REPORT
A 26-year-old primigravida with history of 3 months of amenorrhea was struck by lightning as she was standing beside a tree which left her unconscious. She was immediately taken to the emergency department of Maharana Bhupal Govt Hospital (MBGH Hospital), Udaipur, Rajasthan, where she was assessed and admitted in ICU under Department of Medicine.
On examination, her clothes were partially burned. Her vitals on admission were blood pressure 84/56 mmHg, respiratory rate 30 cycles/min, pulse rate 132 beats/min and of low volume. She was put on vasopressor support and was maintaining saturation with 10 L oxygen via face mask. Her Glasgow Coma Scale (GCS) was E2V1M5, pupils were reactive bilaterally and bilateral plantar was extensor, suggestive of brain insult.
Entry wound was from right ear and the exit wound was on abdomen (Fig. 1 a and b). Examination revealed linear first- and superficial second-degree burns. Some blisters were noted on a line traversing from the right ear to abdomen.

Figure 1 a and b. Entry and exit wounds.
The electrocardiogram (ECG) showed deep and symmetrical T-wave inversion in precordial and lateral leads (Fig. 2). There was an associated elevation of troponin T levels (peak: 432 ng/L), suggestive of myocarditis. Laboratory investigations revealed a normal blood count (Hemoglobin – 13 g/dL, white blood cell [WBC] - 13,200, platelet count - 1,80,000), normal renal (Urea - 36, creatinine - 1.24) and liver function tests (SGOT - 38, SGPT - 45, ALP - 54, total protein - 7.4, albumin - 2.8) and no electrolyte abnormalities.
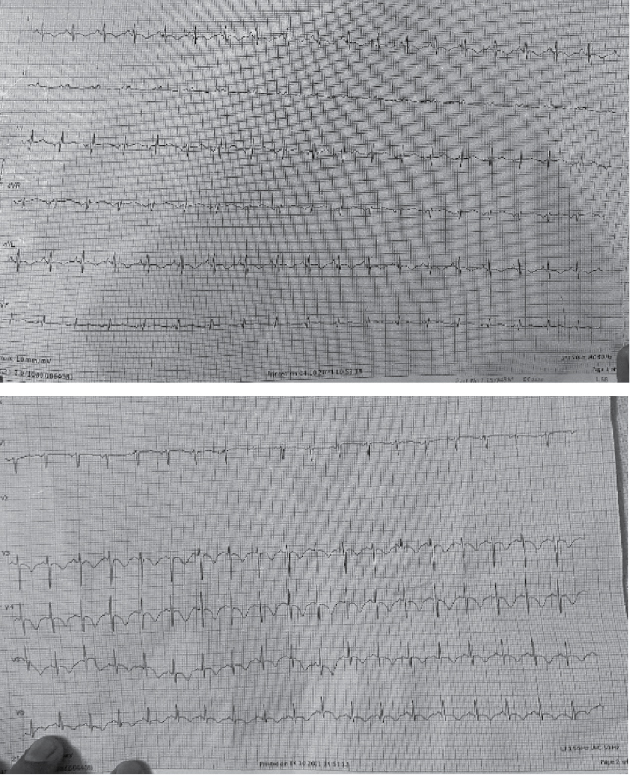
Figure 2. ECG of the patient.
A transthoracic echocardiography revealed reduced ejection fraction of the left ventricle to 25% with global left ventricle hypokinesia, moderate mitral regurgitation and tricuspid regurgitation.
On third day, she started obeying commands and taking food orally, but complained of difficulty in hearing. She was referred to the Department of ENT. On otoscopic examination, she was found to have rupture of tympanic membrane bilaterally. Pure tone audiometry revealed bilateral moderate-to-severe mixed type of hearing loss (Fig. 3) and the patient was advised tympanoplasty.
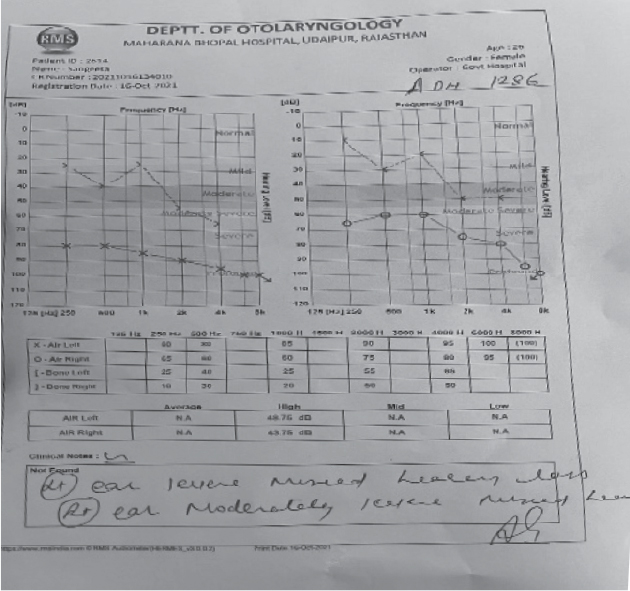
Figure 3. Mixed type hearing loss on audiometry.
On the same day, she complained of bleeding per vagina for which she was referred to Department of OBG. Patient had missed abortion and was terminated medically.
The cardiopulmonary function was monitored at the ICU for 4 days. Hemodynamic parameters became stable and she was weaned off from vasopressor and oxygen support.
She was shifted to medicine ward and noncontrast computed tomography (NCCT) head was done, which did not reveal any significant abnormality.
For the burn injuries, the patient underwent conservative management. Dressing was changed daily using a paraffin gauze dressing and topical hyaluronate. She was discharged from the hospital after 7 days and advised to follow-up in medicine OPD.
DISCUSSION
Lightning injuries are categorized primarily into direct strikes, side splash, contact injury and ground current. Ground current accounts for about 50% of cases of lightning injuries and occurs when the lightning strikes near an individual and travels to the person via ground. Side splash accounts for about one-third of cases and occurs when lightning strikes nearby and jumps to a person.
Contact injury occurs when an individual is touching an object that has been struck by lightning. Direct strikes account for just 5% of these injuries and occur when lightning directly strikes an individual.
The mechanism of lightning injuries may include electrical injury, burns due to heat and mechanical trauma. Lightning injury is diagnosed on the basis of history of the injury and examination.3 A direct strike can cause lethal injuries.
Lightning strike patients can present with injuries to several organ systems. Neurological and cardiological complications have often been reported with lightning strike.4
The common injuries associated with lightning strike include burns, cardiovascular disorders, neurological disorders, kidney failure and psychological trauma.
Cardiological manifestations of a lightning strike may include myocardial necrosis and rhythm abnormalities. Cardiac arrest and ventricular fibrillation usually have lethal consequences if the patient is not immediately resuscitated. ECG may show mimicking acute coronary syndrome, arrhythmias, myocarditis. Takotsubo cardiomyopathy has been reported following lightning strike.2
Neurological manifestations after a lightning strike can range from transient benign symptoms to permanent damage. There may be a temporary loss of consciousness, amnesia, paresis, encephalopathy, etc. Electric current can damage the structural integrity of nerve membranes and muscle tissues.5
Burns caused due to a lightning strike are usually superficial second-degree burns and extensive tissue damage or large cutaneous burns are rarely seen. Management of such patients is the same as any other burn victim.
A characteristic skin alteration seen in patients with lightning injuries are Lichtenberg figures, where a transient reddish, fern-like pattern develops on the skin due to lightning strike.6,7
Renal failure can be seen in patients with lightning strike on account of myoglobinuria.8 Renal function of patients struck by lightning should monitored regularly. Our patient had transient episode of oliguria which subsided with fluid therapy.
Psychological impairment is also possible in patients with lightning injury. The neuropsychological and cognitive deficits seen in these patients resemble those observed in traumatic brain injury or post-traumatic stress disorder.8
CONCLUSION
This case describes multi-organ injuries in a patient struck by lightning and emphasizes the need for evaluating all possible injuries that can occur due to lightning. Interdisciplinary management of multi-organ injuries due to lightning strike is highly important for early detection and management of the injury.
REFERENCES
- Whitcomb D, Martinez JA, Daberkow D. Lightning injuries. South Med J. 2002;95(11):1331-4.
- Dundon BK, Puri R, Leong DP, Worthley MI. Takotsubo cardiomyopathy following lightning strike. BMJ Case Rep. 2009;2009:bcr03.2009.1646.
- Jensen JD, Thurman J, Vincent AL. Lightning injuries. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK441920/.
- Gruhn KM, Knossalla F, Schwenkreis P, Hamsen U, Schildhauer TA, Tegenthoff M, et al. Neurologische Erkrankungen nach Blitzschlag: Lightning strikes twice [Neurological diseases after lightning strike: Lightning strikes twice]. Nervenarzt. 2016;87(6):623-8. German.
- Lee RC, Zhang D, Hanning J. Biophysical injury mechanisms in electrical shock trauma. Annu Rev Biomed Eng. 2002;2:477-509.
- Mahajan AL, Rajan R, Regan P. Lichtenberg figures: cutaneous manifestation of phone electrocution from lightning. J Plast Reconstr Aesthet Surg. 2008;61(1):111-3.
- Resnik BI, Wetli CV. Lichtenberg figures. Am J Forensic Med Pathol. 1996;17(2):99-102.
- Cherington M. Neurologic manifestations of lightning strikes. Neurology. 2003;60(2):182-5.