Published in IJCP
October 2022
Review Article
Sodium-glucose Co-transporter 2 Inhibitors: A Novel Molecule for Health Care Practitioners in Diabetology, Cardiology and Nephrology
October 13, 2022 | AG Unnikrishnan, Kamlesh Khunti, Tiny Nair, Aravinda Jagadeesh, Vedavati Purandare
Diabetes & Endocrinology
Abstract
Prevention and timely management of cardiovascular (CV) complications like myocardial infarction, heart failure (HF), stroke and renal complications, like chronic kidney disease (CKD) and end-stage renal disease, are important to improve the quality of life and survival in people with type 2 diabetes mellitus (T2DM). The multifaceted action of sodium-glucose co-transporter 2 inhibitors (SGLT2i) results in effective glycemic control with benefits on CV and renal risk factors, like body weight, blood pressure, uric acid and albuminuria. Robust CV and renal event reduction is reflected in the outcomes of large CV outcome trials, meta-analyses and real-world studies. Recent evidence has proven cardiac and renal benefits with SGLT2i in subjects with HF and CKD irrespective of their T2DM status. Until recently, SGLT2i was used as a glucose-lowering molecule with pleiotropic benefits, mainly by primary care practitioners and diabetologists. The potential for cardiac and renal protection in people with and without T2DM has shifted an interest in cardiologists and nephrologists to view it as a cardiac and renal molecule, respectively. Thus, the role of SGLT2i in the management of T2DM is undergoing a paradigm shift—straddling the interfaces of diabetology, cardiology, nephrology and primary care—moving away from being considered a pure antidiabetic molecule. We conducted a literature review of SGLT2i in management of T2DM along with their protective effects on CV and renal parameters in patients with or without baseline comorbidities.
Keywords: Cardiologist, diabetologist, nephrologist, primary care practitioners, SGLT2 inhibitors, type 2 diabetes mellitus
People with type 2 diabetes mellitus (T2DM) experience considerable micro- and macrovascular complications.1 Cardiovascular disease (CVD), the main macrovascular complication (>30%) in subjects with T2DM, leads to subclinical or even overt heart failure (HF) (14.9%), with increased mortality (9.9%).2 Additionally, silent coronary ischemia 10% to 20% in diabetics vs. 1% to 4% in nondiabetics3 makes the T2DM population vulnerable to an increased morbidity and mortality. The American Diabetes Association (ADA) recommends calculating the 10-year atherosclerotic cardiovascular disease (ASCVD) risk, besides including strong measures, like diet modification and tight control of blood pressure (BP) and lipid levels to reduce CVD.4 Several large studies have documented that conventional therapies are unable to reduce the macrovascular complications.5,6
Sodium-glucose co-transporter 2 inhibitors (SGLT2i) have demonstrated an improvement in cardiovascular (CV) outcomes. SGLT2i have reduced the rate of hospitalization for heart failure (HHF) and CV death in patients with or without pre-existing HF or ASCVD.7-9 Along with CVD protection, trials with SGLT2i have demonstrated renal protection. Diabetic kidney disease (DKD)—a leading cause of chronic kidney disease (CKD) and end-stage renal disease (ESRD)—occurs in ~40% of people with T2DM and is additionally associated with increased CVD.10 SGLT2i have shown renal protection in multiple large cardiovascular outcome trials (CVOTs), which depict CV safety of this class of drugs with encouraging results on albuminuria and ESRD outcomes.7,11-14 These renal benefits and recommendations are causing nephrologists to change their perception of SGLT2i in being just glucose-lowering drugs (GLDs). This review aims to provide an overview of SGLT2i dynamics in clinical practice from the perspective of diabetologists, cardiologists, nephrologists and primary care practitioners (PCPs).
Methodology
We searched for published literature on PubMed and Embase databases using the keywords – “type 2 diabetes mellitus”, “sodium-glucose co-transporter 2 inhibitor”, “SGLT2 inhibitor”, “dapagliflozin”, “canagliflozin”, “empagliflozin”, “efficacy” and “safety”, etc. Instead of following systematic literature review methodology (using checklists and systematic screening), we focused on our specific area of priority. The data published up to November 2020 with language restriction in English were considered. Conference abstracts and available results from clinicaltrials.gov database were hand searched. The references cited in all the above retrieved publications were also reviewed for relevance and were obtained when applicable.
Mechanism of Action
What Makes it an Molecule for Diabetologists?
The unique insulin-independent action of SGLT2i contributes to minimal hypoglycemia and a low potential for beta-cell exhaustion.15 The enhanced insulin sensitivity and innate insulin release from beta cells can reduce the need for external insulin injections and expenses associated with insulin therapy.16 Randomized controlled trials have shown that SGLT2i therapy reduces insulin resistance17 (p < 0.001) and improves insulin sensitivity18 (p = 0.0059). SGLT2i may play a role even in advanced T2DM stages, characterized by irreparable decline in beta-cell function, because of their insulin independent mechanism.19
The ADA 2021 guidelines4 recommend SGLT2i as the first-line treatment after metformin if there is a compelling indication to minimize hypoglycemia or weight gain, or to encourage weight loss. The European Society of Cardiology/European Association for the Study of Diabetes (ESC/EASD) guidelines place SGLT2i before metformin with a IA recommendation for empagliflozin, canagliflozin or dapagliflozin in subjects with T2DM and CVD or at very high or high CV risk to reduce CV events – with an recommendation for empagliflozin use in T2DM with CVD to reduce the risk of death.20
What Makes it an Molecule for Cardiologists?
What attracts physicians and cardiologists is the positive impact of SGLT2i on CV comorbidities; efficacy in subjects with risk factors for CVD, alongside benefits in subjects with HF (with and without T2DM). Although the precise mechanism of CV benefits of SGLT2is is still under scrutiny, they are likely to be due to the hemodynamic and metabolic effects unrelated to their glucose-lowering efficacy.21 Both ADA4 and ACC/American Heart Association (AHA) guidelines22 recommend the first-line addition of SGLT2i when ASCVD predominates, for reducing CV risk (secondary prevention), while the Food and Drug Administration (FDA) approval for dapagliflozin use in T2DM with multiple CV risk factors (along with those with established CVD [eCVD]) to reduce the risk of HHF suggests a primary preventive role in subjects with T2DM.23
Hemodynamic effects
High BP is a known CV risk factor; hence, lowering BP in T2DM population reduces CV events. The mechanism of BP reduction with SGLT2i occurs by osmotic diuresis and a lower sympathetic tone. The latter mechanism lowers BP, without causing a compensatory increase in heart rate.24 Several studies have explored the adaptive ketogenesis theory, reduction in body weight and arterial stiffness to explain the BP-lowering benefit.25,26 SGLT2i also inhibit the heart Na+-H+ exchanger, thereby improving mitochondrial function, reducing cardiac remodeling and enhancing heart function.27
Metabolic effects
Metabolic benefits with SGLT2i in cardiac protection include a lower risk for hypoglycemia; adaptive ketogenesis; calorie restriction mimicry and improvement in body weight and lipid and uric acid levels. The lower incidence of hypoglycemia with SGLT2i is because of their insulin-independent mode of action, which also aids in reducing the CV risk.28 Adaptive ketogenesis with increased ketones occurs with SGLT2i use because of the elevated glucagon levels. Ketones are an efficient fuel source for the ischemic heart, with added benefits of reducing free-radical injury, resulting in a better cardiac function.29 Reduction in body weight and waist circumference has a positive impact on CV outcomes and insulin resistance.30 A dose-dependant reduction in body weight of 1.6-2.5 kg was shown in a meta-analysis, while another study demonstrated that this weight reduction could be sustained at the 4-year follow-up.31,32 The preferential loss of visceral and subcutaneous fats compared with lean tissue is a benefit.33
Elevated uric acid levels are a CV risk factor and mediate renal damage. The loss of uric acid in urine due to the inhibition of absorption in the renal proximal convoluted tubule by SGLT2i enables the reduction of CV risk and slows CKD progression.11,34 Hematocrit improvement (2-4%) has been consistently seen with SGLT2i use, even in patients with CKD (except stage 4 CKD). This improvement is attributed to an enhanced erythropoietin levels. Elevated hematocrit levels may correct sympathetic hyperactivity in T2DM leading to a reduction in CV mortality and risk for HHF.35 SGLT2is also favorably affect albuminuria, a CV risk factor, by restoring the tubuloglomerular feedback and reducing intraglomerular pressure.36 An improvement in albuminuria translates into cardiac and renal protection.
Benefits in subjects with heart failure
People with T2DM are at a high risk for developing HF with reduced ejection fraction (HFrEF) or HF with preserved ejection fraction (HFpEF) and renal hypoxia leading to new-onset HF or HF progression.20,37 SGLT2i action reduces sympathetic outflow to the heart, lowering cardiac wall stress, fibrosis and volume overload.37 The HHF endpoint being the most sensitive to SGLT2i use in the completed CVOTs led to the theory that SGLT2i reduce CV events mainly by HF prevention rather than atherothrombosis inhibition.38 SGLT2i can reduce morbidity and mortality in pure HF patients with or without comorbid diabetes. Ongoing SGLT2i trials in HF may confirm if it is a class effect. The CANOSSA trial in subjects with T2DM and HFpEF reported improved endothelial and diastolic functions with canagliflozin. HF markers like atrial natriuretic peptide (p = 0.0001), brain natriuretic peptide (p < 0.0001) and ejection fraction (EF) (p = 0.005) improved at 12 months compared with baseline.39
The EMPA-HEART trial40 showed benefits on left ventricular remodeling in T2DM patients with eCVD. The improvement in left ventricular mass index (-2.6 vs. 0.01 g/m2, p = 0.01) at 6 months mechanistically explained the HF benefits demonstrated in the EMPA-REG OUTCOME trial. The DAPA-HF8 trial with dapagliflozin demonstrated a reduction in the composite of HHF or CV death or urgent HF visit (hazard ratio [HR]: 0.74; 95% confidence interval [CI]: 0.65-0.85; p < 0.001), HHF (HR: 0.70; 95% CI: 0.59-0.83), CV death (HR: 0.82; 95% CI: 0.69-0.98), and all-cause death (HR: 0.83; 95% CI: 0.71-0.97) in HFrEF patients with (42%) and without T2DM. DEFINE-HF results demonstrated a clinically meaningful improvement in the dual primary outcome of HF-related quality of life or natriuretic peptides (61.5%, dapagliflozin vs. 50.4%, placebo, adjusted odds ratio: 1.8, 95% CI: 1.03-3.06, p = 0.039), with similar results in subjects with or without T2DM.41 The EMPEROR-Reduced trial reported a significant reduction in the composite of CV death and HHF (HR: 0.75; 95% CI: 0.65-0.86; p < 0.001) with consistent benefits in subjects with (49.8%) and without T2DM. These benefits with empagliflozin may broaden the target HF patient group to advanced New York Heart Association stages, as most participants (73%) had an EF <30%.9
The ADA 2021 guidelines already recommend SGLT2i as the first-line therapy in subjects with T2DM and comorbid HF.4 The FDA approved dapagliflozin to reduce risk of HF in adults with T2DM and multiple CV risk factors or with eCVD.42
What Makes it an Molecule for Nephrologists?
The renal benefits, evidenced by the reduction in albuminuria, slowdown in progression to ESRD and reduced need for renal replacement therapy (RRT), are mediated by several mechanisms.7,11-13 Increased sodium access to the macula densa due to SGLT2 inhibition lowers the intraglomerular pressure, decreases albuminuria and possibly slows the decline of kidney function in people with diabetes.42 Hypoxia in the milieu of proximal convoluted tubule is alleviated as SGLT2is reduce oxygen consumption by the Na+/K+ pump in the epithelial cells.35 Reduction in sympathetic outflow to the kidney by SGLT2i action reduces the renin-angiotensin-aldosterone system (RAAS) activity and corrects fluid overload. Adaptive ketogenesis by SGLT2i action improves renal function by ensuring a more efficient metabolic substrate like ketones.43 EMPA-REG OUTCOME, CANVAS and DECLARE-TIMI 58 trials demonstrated improved renal outcomes, albeit as secondary endpoints with empagliflozin, canagliflozin and dapagliflozin.7,11,12
In the CREDENCE study involving T2DM subjects with albuminuric CKD, canagliflozin significantly reduced the composite of ESRD, a doubling of serum creatinine level or death from renal or CV causes by 30%.13 DAPA-CKD results reported a significant impact (HR: 0.61; 95% CI: 0.51-0.72; p < 0.001) of dapagliflozin on the composite primary outcome of sustained decline in the estimated glomerular filtration rate (eGFR) of at least 50%, ESRD or death from renal or CV causes in subjects with CKD (n = 4,304) – with or without T2DM. This extension of benefit to pure CKD patients without T2DM (32.5%), and to patients with lower eGFR threshold (14.5% had eGFR <30 mL/min/1.73 m2) confirmed renal protection in a broader group of patients. Moreover, a reduction was seen in the composite of sustained decline in eGFR of at least 50%, ESRD or death from renal causes (HR: 0.56; 95% CI: 0.450.68; p < 0.001), the composite of CV death or HHF (HR: 0.71; 95% CI: 0.55-0.92; p = 0.009), and mortality (HR: 0.69; 95% CI: 0.53-0.88; p = 0.004).14
Significant improvement in the urine albumin-creatinine ratio was seen with dapagliflozin vs. placebo in the DELIGHT trial44 (−21.0%; 95% CI: −34.1, −5.2; p = 0.011) on follow-up at the end of 24 weeks while in the DERIVE trial,45 a significant reduction at week-12 (−41.7%; 95% CI: −57.1, −21.0; p < 0.001) was maintained, but did not reach significance at week-24 (−14.0%; 95% CI: −42.3, 28.0; p = 0.454). Ertugliflozin revealed glycemic efficacy and an acceptable safety profile in 468 subjects with T2DM and stage 3 CKD over a 52-week period in the VERTIS-RENAL trial.46
However, the VERTIS-CV trial with ertugliflozin did not show a significant benefit for the renal composite endpoint (secondary endpoint) of death from renal causes, RRT or doubling of serum-creatinine level.47 The ACC 2018 consensus pathway on novel therapies recommends the first-line addition of SGLT2i to metformin in T2DM and CKD subjects, with or without ASCVD, provided there is no ESRD.21 The ADA 2021 guidelines4 also recommend SGLT2i as a preferable option when CKD predominates. Canagliflozin received FDA approval for use in subjects with DKD (with albuminuria) to reduce the risk of ESRD, worsening of renal function, CV death and HHF.48 Thus, the question remains – should SGLT2i form a targeted treatment option for DKD? SGLT2is with their multifaceted action at the level of the pancreas, heart and kidney, allow PCPs, diabetologists, cardiologists and nephrologists to provide multiorgan-targeted benefits for subjects with T2DM (Fig. 1).
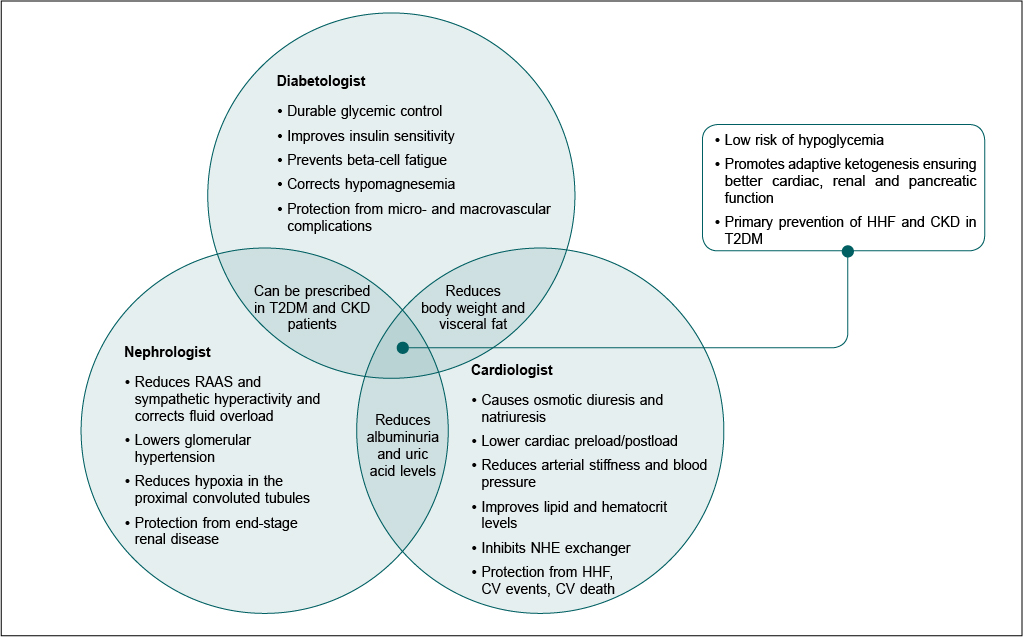
Figure 1. SGLT2i benefits for a diabetologist, cardiologist and nephrologist.
CKD = Chronic kidney disease; CV = Cardiovascular; HHF = Hospitalization for heart failure; NHE = Sodium-hydrogen exchanger; RAAS = Renin-angiotensin-aldosterone system; T2DM = Type 2 diabetes mellitus.
Evidence With Sglt2i For Diabetologists, Cardiologists And Nephrologists
Evidence from Randomized Controlled Trials
Table 1 summarizes the main CV and renal endpoints in the landmark CVOTs with SGLT2i. In EMPA-REG OUTCOME, the empagliflozin group demonstrated lower rates of 3-point major adverse cardiac events (MACE), death from CV causes, HHF and death from any cause.49 EMPA-REG renal analysis demonstrated a reduction in the composite of incident or worsening nephropathy (HR: 0.61, 95% CI: 0.53-0.70), progression to macroalbuminuria (HR: 0.62, 95% CI: 0.54-0.72), serum-creatinine doubling (HR: 0.56, 95% CI: 0.39-0.79), and RRT initiation (HR: 0.45, 95% CI: 0.21-0.97).11
|
Table 1. Summary of Cardiovascular and Renal Benefits with SGLT2i
|
| |
EMPA-REG OUTCOME (n = 7,020, T2DM)
|
CANVAS
(n = 10,142, T2DM)
|
DECLARE-TIMI 58
(n = 17,160, T2DM)
|
CREDENCE
(n = 4,401, T2DM with albuminuric CKD)
|
|
Patients with established CVD (n, %)
|
7,020 (100%)
|
6,656 (66%)
|
6,974 (40.6%)
|
2,220 (50.4%)
|
|
Follow-up (years)
|
3.1
|
2.4
|
4.2
|
2.62
|
|
SGLT2i
|
Empagliflozin 10 or 25 mg vs. placebo daily
|
Canagliflozin 100 or 300 mg vs. placebo daily
|
Dapagliflozin 10 mg vs. placebo daily
|
Canagliflozin 100 mg vs. placebo daily
|
|
Primary endpoint: Composite of CV death, MI or stroke
|
HR: 0.86 (0.74-0.99),
p < 0.001 for NI, p = 0.04 for superiority
|
HR: 0.86 (0.75-0.97) NI,
p < 0.001
Superiority, p = 0.02
|
HR: 0.93 (0.84-1.03)
NI, p < 0.001
Superiority, p = 0.17
|
HR: 0.80 (0.67-0.95),
p = 0.01
|
|
CV death
|
HR: 0.62 (0.49-0.77),
p < 0.001
|
HR: 0.87 (0.72-1.06),
p = NS
|
HR: 0.98 (0.82-1.17),
p = NS
|
HR: 0.78 (0.61-1.00),
p = 0.05
|
|
HHF
|
HR: 0.65 (0.50-0.85),
p = 0.002
|
HR: 0.67 (0.52-0.87),
p = NS
|
HR:0.73 (0.61-0.88),
p = 0.005
|
HHF: 0.61 (0.47-0.80), p < 0.001
|
|
All-cause mortality
|
HR: 0.68 (0.57-0.82),
p < 0.001
|
HR: 0.87 (0.74-1.01),
p = NS
|
HR: 0.93 (0.82-1.04), p= NS
|
HR: 0.83 (0.68-1.02),
p = NS
|
|
Worsening nephropathy*
|
HR: 0.61 (0.53-0.70)
p < 0.001
|
HR: 0.60 (0.47-0.77)
|
HR: 0.76 (0.67-0.87)
|
HR: 0.66 (0.53-0.81),
p < 0.001
|
*Worsening nephropathy was defined as doubling of serum creatinine level and an eGFR of ≤45 mL/min/1.73 m2, the need for continuous renal-replacement therapy or death due to renal events in EMPA-REG OUTCOME; 40% reduction in eGFR, renal-replacement therapy or death from renal causes in CANVAS; sustained decrease of ≥40% in eGFR to <60 mL/min/1.73 m2, new end-stage renal disease or death from renal or CV causes in DECLARE-TIMI 58; end-stage kidney disease, doubling of serum creatinine or renal death in CREDENCE.
CKD = Chronic kidney disease; CV = Cardiovascular; CVD = Cardiovascular disease; eGFR = Estimated glomerular filtration rate; HHF = Hospitalization for heart failure; HR = hazard ratio; MI = Myocardial infarction; NI = Noninferiority; NS = Nonsignificant; SGLT2i = Sodium-glucose co-transporter 2 inhibitor; T2DM = Type 2 diabetes mellitus.
A recent post hoc analysis of EMPA-REG study observed consistent CV and renal benefits among all Kidney Disease Improving Global Outcomes (KDIGO) categories confirming benefits across the CKD spectrum.50 In the CANVAS program, the canagliflozin group demonstrated lower rates of 3-point MACE, CV death, all-cause mortality and HHF with no heterogeneity of treatment effect across primary and secondary prevention groups and a significant reduction in albuminuria progression (HR: 0.73, 95% CI: 0.67-0.79).49
In the DECLARE-TIMI 58 trial of 17,160 patients, 10,186 patients did not have eCVD, but they had multiple risk factors for ASCVD. Dapagliflozin achieved the MACE criterion for noninferiority, with therapy results demonstrating lower risks for HHF (HR: 0.73, 95% CI: 0.61-0.88) and renal events (HR: 0.76, 95% CI: 0.67-0.87).7 The CREDENCE trial with canagliflozin in subjects with T2DM and albuminuric CKD demonstrated a significant reduction in the primary outcome of composite of ESRD, serum creatinine doubling or death from renal or CV causes (HR: 0.70, 95% CI: 0.59-0.82, p < 0.00001), in addition to a reduction in the risk of CV death, myocardial infarction or stroke, and HHF.13 It showed that the CV and renal benefits were observed even at lower eGFR levels (30-45 mL/min/1.73 m2), suggesting that SGLT2i can be used in more severe stages of CKD.
Evidence from Systematic Review and Meta-analyses and Post Hoc Analyses
A systemic review and meta-analyses (SRMA) of EMPA-REG OUTCOME, CANVAS and DECLARE-TIMI 58 trials showed a significant reduction in MACE (HR: 0.86, 95% CI: 0.80-0.93, p = 0.0014) with SGLT2i in those with eCVD. Further, a 45% reduction in renal disease progression was also seen to be similar in subjects with and without ASCVD.51
Another SRMA confirmed SGLT2i benefits by demonstrating a significant reduction in CV outcomes (relative risk [RR]: 0.81, 95% CI: 0.70-0.94) and renal outcomes (composite renal outcome, HR: 0.71, 95% CI: 0.53-0.95) in subjects with T2DM and CKD, with a mitigation in the annual decline in eGFR slope (difference of 1.35 mL/min/1.73 m2/year; 95% CI: 0.78-1.93).52 Another SRMA reported consistency of SGLT2i effect across trials and different levels of eGFR (baseline eGFR 30-45 mL/min/1.73 m2) and albuminuria with a reduction in the risk of dialysis, transplantation or death due to renal causes (RR: 0.67, 95% CI: 0.52-0.86, p = 0.0019), ESRD (HR: 0.65, 95% CI: 0.53-0.81, p < 0.0001) and acute kidney injury (HR: 0.75, 95% CI: 0.66-0.85, p < 0.0001).53 A prespecified meta-analysis of the EMPEROR-Reduced and DAPA-HF trials reported significant reductions in the all-cause death (HR: 0.87; 95% CI: 0.77-0.98; p = 0.018), CV death (HR: 0.86; 95% CI: 0.76-0.98; p = 0.027), and composite renal outcome (HR: 0.62; in patients with HFrEF, with benefits consistent across subgroups, such as age, sex, diabetes and baseline eGFR.54
Real-world Evidence
In CVD-REAL55 (n = 3,09,056), the use of SGLT2i (n = 1,54,528) versus other GLDs demonstrated a lower risk for HHF (HR: 0.61, 95% CI: 0.51-0.73, p < 0.001), death (HR: 0.49, 95% CI: 0.41-0.57, p < 0.001); and HHF or death (HR: 0.54, 95% CI: 0.48-0.60, p < 0.001) without a country-wise difference. An analysis of the CVD-REAL study (n = 1,53,078) reported that SGLT2i use was associated with a lower risk of mortality in patients with (HR: 0.56, 95% CI: 0.44-0.70) and without (HR: 0.56, 95% CI: 0.50-0.63) CVD. Furthermore, HF (HR: 0.72, 95% CI: 0.63-0.82 and HR: 0.61, 95% CI: 0.48-0.78, with and without CVD, respectively) and the composite of HF or death (HR: 0.63, 95% CI: 0.57-0.70 and HR: 0.56, 95% CI: 0.50-0.62, with and without CVD, respectively) were lowered significantly.56
Preliminary results of the EMPRISE study demonstrated a 50% risk reduction with empagliflozin in HF discharge diagnosis in the primary position (HHF-specific) (HR: 0.50, 95% CI: 0.28-0.91) and 49% in HF discharge diagnosis in any position (HHF-broad) (HR: 0.51, 95% CI: 0.390.68) compared with sitagliptin. The results were consistent for both doses of empagliflozin (10 and 25 mg) and irrespective of the baseline CVD status.57
The CVD-REAL 3 study showed a lower risk of eGFR decline (difference in slope 1.53 mL/min/1.73 m2, 95% CI: 1.34-1.72, p < 0.0001) and renal outcomes (HR: 0.49, 95% CI: 0.35-0.67, p < 0.0001) in the group receiving SGLT2i.58
Emerging Evidence in Chronic Heart Failure with HFrEF and HFpEF
Table 2 shows emerging evidence with multiple phase 2/3 and 4 trials evaluating SGLT2i in subjects with pure HF (HFrEF and HFpEF), without comorbid T2DM, on parameters like cardiac biomarkers, exercise capacity, quality of life, echocardiographic features, HF symptoms, worsening HF and CV death. These study results may elevate the importance of SGLT2i in the clinical practice of a cardiologist.
|
Table 2. Phase 2/3/4 Trials Evaluating SGLT2i in HF
|
|
Trial (NCT Number)
|
Study population
|
Expected outcomes
|
Study status
|
|
Phase 2 trial evaluating SGLT2i in HF
|
|
EMPIRE-HF (NCT03198585)
|
190 participants
Stable, symptomatic HFrEF (LVEF ≤40%)
|
Evaluate empagliflozin 10 mg on cardiac biomarkers, cardiac function at rest, at stress and during exercise, renal function, metabolism, daily activity and health-related QoL
|
Completed: January 2020*
|
|
Phase 3 trials evaluating SGLT2i in HFrEF
|
|
EMPERIAL-Reduced (NCT03448419)
|
312 participants
Chronic HFrEF LVEF ≤40%
|
Evaluate empagliflozin 10 mg vs. placebo on exercise capacity using 6MWT
|
Completed: October 2019
|
|
DETERMINE-Reduced (NCT03877237)
|
313 participants
HF (NYHA class II-IV) with reduced ejection fraction defined as LVEF ≤40%
|
Evaluate dapagliflozin 10 mg on exercise capacity in patients with HFrEF (LVEF ≤40%)
|
Completed: March 2020*
|
|
Phase 3 trials evaluating SGLT2i in HFpEF
|
|
EMPERIAL-Preserved (NCT03448406)
|
315 participants
Chronic HFpEF (NYHA class II-IV) LVEF >40%
|
Evaluate empagliflozin 10 mg vs. placebo on exercise ability using 6MWT
|
Completed: October 2019*
|
|
DETERMINE-Preserved (NCT03877224)
|
504 participants
Chronic HFpEF (NYHA class II-IV) LVEF >40%
|
Evaluate dapagliflozin 10 mg on exercise capacity using 6MWT
|
Completed: July 2020*
|
|
EMPEROR-Preserved (NCT03057951)
|
5,988 participants
Chronic HFpEF (NYHA class II-IV) LVEF >40%
|
Evaluate efficacy and safety of empagliflozin 10 mg vs. placebo on top of guideline-directed medical therapy
|
April 2021
|
|
DELIVER (NCT03619213)
|
6,100 participants
HFpEF (NYHA class II-IV) with LVEF >40%
|
Evaluate dapagliflozin 10 mg on reducing CV death or worsening HF
|
November 2021
|
|
Phase 4 trials evaluating SGLT2i in HF
|
|
EMBRACE-HF (NCT03030222)
|
60 participants
NYHA class II-IV
HFpEF (LVEF >40%) or HFrEF (LVEF ≤40%) ischemic or nonischemic etiology who already have a CardioMEMs device
|
Evaluate empagliflozin 10 mg on hemodynamic parameters (pulmonary artery diastolic pressures)
|
October 2020 (not recruiting)
|
|
PRESERVED-HF (NCT03030235)
|
320 participants
Dyspnea (NYHA class II-IV) without evidence of a noncardiac or ischemic explanation for dyspnea
LVEF ≥45%
|
Evaluate dapagliflozin 10 mg on HF-specific biomarkers (NTproBNP and BNP), symptoms, health status and QoL
|
February 2021
|
*Results not published
BNP = Brain natriuretic peptide; CV = Cardiovascular; HF = Heart failure; HFpEF = Heart failure with preserved ejection fraction; HFrEF = Heart failure with reduced ejection fraction; LVEF = Left ventricular ejection fraction; NTproBNP = N-terminal pro-B-type natriuretic peptide; NYHA = New York Heart Association; QoL = Quality of life; SGLT2i = Sodium-glucose co-transporter 2 inhibitor; T2DM = Type 2 diabetes mellitus; 6MWT = 6-minute walk test.
Emerging Evidence with SGLT2i for Coexistent T2DM and HF
Several trials currently investigating the benefits of SGLT2i in subjects with the dual burden of T2DM and HF are described in Table 3. These trials will assess the mechanisms and effects of SGLT2i on exercise capacity, systolic and diastolic cardiac function, and HF biomarkers when T2DM and HF coexist, and their results may augment the importance of SGLT2i in the practice of diabetologists and cardiologists.
|
Table 3. Emerging Evidence with SGLT2i in HF with T2DM and CKD With and Without T2DM
|
|
Trial (NCT number)
|
Sample size
|
Study objective and population
|
Study status
|
|
In subjects with T2DM and HF
|
|
Treatment of DM in HFrEF (NCT02920918)
|
36
|
Evaluate canagliflozin 100 mg vs. sitagliptin 100 mg on exercise capacity, cardiac function and cardiac biomarkers in HFrEF (EF ≤40%)
|
Completed*: September 2018
|
|
RECEDE-CHF (NCT03226457)
|
23
|
Compare empagliflozin 25 mg, to placebo in patients with T2DM and chronic HF (NYHA II/III) with left ventricular systolic dysfunction and who are already on a loop diuretic
|
Completed: January 2019
|
|
ELSI (NCT03128528)
|
84
|
Evaluate empagliflozin 10 mg vs. placebo on reduction of tissue sodium content in patients with chronic HFrEF (<40%) and HFmEF (40-49%) with T2DM
|
Completed: April 2020
|
|
IDDIA (NCT02751398)
|
60
|
Evaluate dapagliflozin on diastolic dysfunction in T2DM patients with ≥ grade 1 diastolic function at resting echocardiography
|
Completed: June 2020
|
|
SOLOIST-WHF (NCT03521934)
|
1,222
|
Evaluate sotagliflozin on clinical outcomes in hemodynamically stable patients with T2DM post-WHF (EF <40%).
|
Terminated prematurely: June 2020
|
|
ERADICATE-HF** (NCT03416270)
|
36
|
Evaluate mechanism by which ertugliflozin 15 mg modifies cardiorenal interactions that regulate fluid volume and neurohormonal activation in T2DM and HF (EF ≥20%).
|
Completion:
March 2021
|
|
EXCEED (UMIN000027095)
|
100 (target)
|
Evaluate ipragliflozin on cardiac function in patients with chronic HF (NYHA I-III) and T2DM vs. non-SGLT2i antidiabetic drugs
|
Completion: Date not available
|
|
In subjects with CKD (with and without T2DM)
|
|
SCORED (NCT03315143)
|
10,584
|
Evaluate sotagliflozin, on time to: a) first MACE or b) CV death or HHF. Patients eligible if T2DM and eGFR ≥25 and ≤60 mL/min/1.73 m2
|
Terminated prematurely: July 2020
|
|
RACELINES (NCT03433248)
|
66
|
Evaluate empagliflozin 10 mg and linagliptin 5 mg monotherapy or combination vs. gliclazide 30 mg on changes in GFR
Patients eligible if T2DM and eGFR ≥45 and on treatment with RAAS blockers
|
Completion: December 2021
|
|
EMPA-KIDNEY (NCT03594110)
|
6,000
|
Evaluate empagliflozin, on composite of time to first occurrence of kidney disease or CV death
Patients eligible if CKD and eGFR ≥20 to <45 or ≥45 to <90 with UACR ≥200 mg/g
|
Completion: October 2022
|
*Results not published; **Not yet recruiting
CKD = Chronic kidney disease; CV = Cardiovascular; DM = Diabetes mellitus; EF = Ejection fraction; eGFR = Estimated glomerular filtration rate; ESRD = End-stage renal disease; HF = Heart failure; HHF = Hospitalization for heart failure; HFmEF = Heart failure with mid-range ejection fraction; HFrEF = Heart failure with reduced ejection fraction; MACE = Major adverse cardiovascular events; NYHA = New York Heart Association; RAAS = Renin-angiotensin-aldosterone system; SGLT2i = Sodium-glucose co-transporter 2 inhibitor; T2DM = Type 2 diabetes mellitus; UACR = Urine albumin-to-creatinine ratio; WHF = Worsening heart failure.
Emerging Evidence with SGLT2i in CKD (With and Without T2DM)
Trials currently investigating SGLT2i in subjects with CKD (with and without T2DM) are described in Table 3. These trials will assess the renal physiology, biomarkers and renal and CV endpoints at different CKD stages. The EMPA-KIDNEY trial59 like the DAPA-CKD trial14 specifically plans to evaluate renal outcomes in CKD subjects without T2DM. Results from these trials may cause a paradigm shift in the practice of nephrologists.
Role Of PCPs For SGLT2i Use
PCPs form the first touch point of care for T2DM in many countries; 90% of people with T2DM were treated by PCPs in the United States.60 In the United Kingdom, only 20% of people with T2DM see a specialist, implying 80% are seen by PCPs.61 T2DM management in primary care is complex with multiple challenges including clinician and patient inertia in ensuring treatment compliance and implementing therapeutic advances.62
A Canadian survey highlighted the importance of PCPs in individualizing treatment decisions when initiating SGLT2i therapy.63 While the PCP role is important in the everyday management, expert evaluation for diabetes-related complications, CV risk and renal status by diabetologists/endocrinologists, cardiologists and nephrologists, is essential to optimize treatment decisions and improve clinical outcomes.64
Conclusion
PCPs, diabetologists and endocrinologists play a prime role as the first contact for most subjects with T2DM and rely on novel therapies like SGLT2i for effective glycemic control and microvascular and macrovascular risk reduction. Cardiologists and nephrologists can play an equally prime role by routinely screening their patients for T2DM, and optimally managing CV and renal risk factors by assimilating SGLT2i use in their clinical practice. SGLT2i offer a meeting point for PCPs, diabetologists, cardiologists and nephrologists by delivering benefits as antidiabetic, cardiac and renal molecules.
Acknowledgment
The authors would like to thank AstraZeneca Pharma India Ltd. for the development of this manuscript in collaboration with Dr Anita Bhat, Covance Scientific Services & Solutions Pvt. Ltd. in accordance with GPP3 guidelines (http://www.ismpp.org/gpp3).
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article and take responsibility for the integrity of the work as a whole and have given their approval for this version to be published.
References
- Orasanu G, Plutzky J. The pathologic continuum of diabetic vascular disease. J Am Coll Cardiol. 2009;53(5 Suppl):S35-42.
- Einarson TR, Acs A, Ludwig C, Panton UH. Prevalence of cardiovascular disease in type 2 diabetes: a systematic literature review of scientific evidence from across the world in 2007-2017. Cardiovasc Diabetol. 2018;17(1):83.
- Leon BM, Maddox TM. Diabetes and cardiovascular disease: epidemiology, biological mechanisms, treatment recommendations and future research. World J Diabetes. 2015;6(13):1246-58.
- American Diabetes Association. 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes—2021. Diabetes Care. 2021;44(Suppl 1):S125-50.
- ADVANCE Collaborative Group, Patel A, MacMahon S, Chalmers J, Neal B, Billot L, Woodward M, et al. Intensive blood glucose control and vascular outcomes in patients with type 2 diabetes. N Engl J Med. 2008;358(24):2560-72.
- American Diabetes Association. Implications of the United Kingdom prospective diabetes study. Diabetes Care. 2002;25(Suppl 1):s28-32.
- Wiviott SD, Raz I, Bonaca MP, Mosenzon O, Kato ET, Cahn A, et al; DECLARE–TIMI 58 Investigators. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2019;380(4):347-57.
- McMurray JJV, Solomon SD, Inzucchi SE, Køber L, Kosiborod MN, Martinez FA, et al; DAPA-HF Trial Committees and Investigators. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381(21):1995-2008.
- Packer M, Anker SD, Butler J, Filippatos G, Pocock SJ, Carson P, et al; EMPEROR-Reduced Trial Investigators. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020;383(15):1413-24.
- Alicic RZ, Rooney MT, Tuttle KR. Diabetic kidney disease: challenges, progress, and possibilities. Clin J Am Soc Nephrol. 2017;12(12):2032-45.
- Wanner C, Inzucchi SE, Lachin JM, Fitchett D, von Eynatten M, Mattheus M, et al. Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med. 2016;375(4):323-34.
- Mahaffey KW, Neal B, Perkovic V, de Zeeuw D, Fulcher G, Erondu N, et al; CANVAS Program Collaborative Group. Canagliflozin for primary and secondary prevention of cardiovascular events: results from the CANVAS program (Canagliflozin Cardiovascular Assessment Study). Circulation. 2018;137(4):323-34.
- Perkovic V, Jardine MJ, Neal B, Bompoint S, Heerspink HJL, Charytan DM, et al; CREDENCE Trial Investigators. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380(24):2295-306.
- Heerspink HJL, Stefánsson BV, Correa-Rotter R, Chertow GM, Greene T, Hou FF, et al; DAPA-CKD Trial Committees and Investigators. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383(15):1436-46.
- Kalra S. Sodium glucose co-transporter-2 (SGLT2) inhibitors: a review of their basic and clinical pharmacology. Diabetes Ther. 2014;5(2):355-66.
- Merovci A, Mari A, Solis-Herrera C, Xiong J, Daniele G, Chavez-Velazquez A, et al. Dapagliflozin lowers plasma glucose concentration and improves β-cell function. J Clin Endocrinol Metab. 2015;100(5):1927-32.
- Ott C, Jumar A, Striepe K, Friedrich S, Karg MV, Bramlage P, et al. A randomised study of the impact of the SGLT2 inhibitor dapagliflozin on microvascular and macrovascular circulation. Cardiovasc Diabetol. 2017;16(1):26.
- Mudaliar S, Henry RR, Boden G, Smith S, Chalamandaris AG, Duchesne D, et al. Changes in insulin sensitivity and insulin secretion with the sodium glucose cotransporter 2 inhibitor dapagliflozin. Diabetes Technol Ther. 2014;16(3):137-44.
- Chaudhury A, Duvoor C, Reddy Dendi VS, Kraleti S, Chada A, Ravilla R, et al. Clinical review of antidiabetic drugs: implications for type 2 diabetes mellitus management. Front Endocrinol (Lausanne). 2017;8:6.
- Cosentino F, Grant PJ, Aboyans V, Bailey CJ, Ceriello A, Delgado V, et al; ESC Scientific Document Group. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J. 2020;41(2):255-323.
- Das SR, Everett BM, Birtcher KK, Brown JM, Cefalu WT, Januzzi JL, et al. 2018 ACC Expert consensus decision pathway on novel therapies for cardiovascular risk reduction in patients with type 2 diabetes and atherosclerotic cardiovascular disease: a report of the American College of Cardiology Task Force on expert consensus decision pathways. J Am Coll Cardiol. 2018;72(24):3200-23.
- American College of Cardiology [Internet]. ACC Endorses New ADA 2019 Standards of Medical Care in Diabetes [cited 2021 Jun 14]. Available from: https://www.acc.org/latest-in-cardiology/articles/2018/12/17/13/34/acc-endorses-new-ada-2019-standards-of-medical-care-in-diabetes
- Prescribing Information [Internet]. FARXIGA® (dapagliflozin) tablets [cited 2021 Jun 14]. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/202293s020lbl.pdf
- Lopaschuk GD, Verma S. Mechanisms of cardiovascular benefits of sodium glucose co-transporter 2 (SGLT2) inhibitors: a state-of-the-art review. JACC Basic Transl Sci. 2020;5(6):632-44.
- Cefalu WT, Stenlöf K, Leiter LA, Wilding JP, Blonde L, Polidori D, et al. Effects of canagliflozin on body weight and relationship to HbA1c and blood pressure changes in patients with type 2 diabetes. Diabetologia. 2015;58(6):1183-7.
- Sjöström CD, Hashemi M, Sugg J, Ptaszynska A, Johnsson E. Dapagliflozin-induced weight loss affects 24-week glycated haemoglobin and blood pressure levels. Diabetes Obes Metab. 2015;17(8):809-12.
- Packer M, Anker SD, Butler J, Filippatos G, Zannad F. Effects of sodium-glucose cotransporter 2 inhibitors for the treatment of patients with heart failure: proposal of a novel mechanism of action. JAMA Cardiol. 2017;2(9):1025-9.
- Kalra S, Ghosh S, Aamir AH, Ahmed MT, Amin MF, Bajaj S, et al. Safe and pragmatic use of sodium-glucose co-transporter 2 inhibitors in type 2 diabetes mellitus: South Asian Federation of Endocrine Societies consensus statement. Indian J Endocrinol Metab. 2017;21(1):210-30.
- Kalra S, Jain A, Ved J, Unnikrishnan AG. Sodium-glucose cotransporter 2 inhibition and health benefits: the Robin Hood effect. Indian J Endocrinol Metab. 2016;20(5):725-9.
- Sato T, Aizawa Y, Yuasa S, Kishi S, Fuse K, Fujita S, et al. The effect of dapagliflozin treatment on epicardial adipose tissue volume. Cardiovasc Diabetol. 2018;17(1):6.
- Zaccardi F, Webb DR, Htike ZZ, Youssef D, Khunti K, Davies MJ. Efficacy and safety of sodium-glucose co-transporter-2 inhibitors in type 2 diabetes mellitus: systematic review and network meta-analysis. Diabetes Obes Metab. 2016;18(8):783-94.
- Del Prato S, Nauck M, Durán-Garcia S, Maffei L, Rohwedder K, Theuerkauf A, et al. Long-term glycaemic response and tolerability of dapagliflozin versus a sulphonylurea as add-on therapy to metformin in patients with type 2 diabetes: 4-year data. Diabetes Obes Metab. 2015;17(6):581-90.
- Pereira MJ, Eriksson JW. Emerging role of SGLT-2 inhibitors for the treatment of obesity. Drugs. 2019;79(3):219-30.
- Thomas MC. Renal effects of dapagliflozin in patients with type 2 diabetes. Ther Adv Endocrinol Metab. 2014;5(3):53-61.
- Sano M, Goto S. Possible mechanism of hematocrit elevation by sodium glucose cotransporter 2 inhibitors and associated beneficial renal and cardiovascular effects. Circulation. 2019;139(17):1985-7.
- Heerspink HJL, Kosiborod M, Inzucchi SE, Cherney DZI. Renoprotective effects of sodium-glucose cotransporter-2 inhibitors. Kidney Int. 2018;94(1):26-39.
- Sano M. A new class of drugs for heart failure: SGLT2 inhibitors reduce sympathetic overactivity. J Cardiol. 2018;71(5):471-6.
- Verma S, McMurray JJV. SGLT2 inhibitors and mechanisms of cardiovascular benefit: a state-of-the-art review. Diabetologia. 2018;61(10):2108-17.
- Sezai A, Sekino H, Unosawa S, Taoka M, Osaka S, Tanaka M. Canagliflozin for Japanese patients with chronic heart failure and type II diabetes. Cardiovasc Diabetol. 2019;18(1):76.
- Verma S, Mazer CD, Yan AT, Mason T, Garg V, Teoh H, et al. Effect of empagliflozin on left ventricular mass in patients with type 2 diabetes mellitus and coronary artery disease: the EMPA-HEART CardioLink-6 randomized clinical trial. Circulation. 2019;140(21):1693-702.
- Nassif ME, Windsor SL, Tang F, Khariton Y, Husain M, Inzucchi SE, et al. Dapagliflozin effects on biomarkers, symptoms, and functional status in patients with heart failure with reduced ejection fraction: the DEFINE-HF Trial. Circulation. 2019;140(18):1463-76.
- Herrington WG, Preiss D, Haynes R, von Eynatten M, Staplin N, Hauske SJ, et al. The potential for improving cardio-renal outcomes by sodium-glucose co-transporter-2 inhibition in people with chronic kidney disease: a rationale for the EMPA-KIDNEY study. Clin Kidney J. 2018;11(6):749-61.
- Mudaliar S, Alloju S, Henry RR. Can a shift in fuel energetics explain the beneficial cardiorenal outcomes in the EMPA-REG OUTCOME Study? A unifying hypothesis. Diabetes Care. 2016;39(7):1115-22.
- Pollock C, Stefánsson B, Reyner D, Rossing P, Sjöström CD, Wheeler DC, et al. Albuminuria-lowering effect of dapagliflozin alone and in combination with saxagliptin and effect of dapagliflozin and saxagliptin on glycaemic control in patients with type 2 diabetes and chronic kidney disease (DELIGHT): a randomised, double-blind, placebo-controlled trial. Lancet Diabetes Endocrinol. 2019;7(6):429-41.
- Fioretto P, Del Prato S, Buse JB, Goldenberg R, Giorgino F, Reyner D, et al; DERIVE Study Investigators. Efficacy and safety of dapagliflozin in patients with type 2 diabetes and moderate renal impairment (chronic kidney disease stage 3A): the DERIVE Study. Diabetes Obes Metab. 2018;20(11):2532-40.
- Grunberger G, Camp S, Johnson J, Huyck S, Terra SG, Mancuso JP, et al. Ertugliflozin in patients with stage 3 chronic kidney disease and type 2 diabetes mellitus: the VERTIS RENAL randomized study. Diabetes Ther. 2018;9(1):49-66.
- Cannon CP, Pratley R, Dagogo-Jack S, Mancuso J, Huyck S, Masiukiewicz U, et al; VERTIS CV Investigators. Cardiovascular outcomes with ertugliflozin in type 2 diabetes. N Engl J Med. 2020;383(15):1425-35.
- Prescribing Information [Internet]. Invokana (canagliflozin) Tablets [cited 2021 Jun 14]. Available from: https://www.janssenlabels.com/package-insert/product-monograph/prescribing-information/INVOKANA-pi.pdf
- Neal B, Perkovic V, Mahaffey KW, de Zeeuw D, Fulcher G, Erondu N, et al; CANVAS Program Collaborative Group. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med. 2017;377(7):644-57.
- Levin A, Perkovic V, Wheeler DC, Hantel S, George JT, von Eynatten M, et al; EMPA-REG OUTCOME Investigators. Empagliflozin and cardiovascular and kidney outcomes across KDIGO risk categories: post hoc analysis of a randomized, double-blind, placebo-controlled, multinational trial. Clin J Am Soc Nephrol. 2020;15(10):1433-44.
- Zelniker TA, Wiviott SD, Raz I, Im K, Goodrich EL, Bonaca MP, et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet. 2019;393(10166):31-9.
- Toyama T, Neuen BL, Jun M, Ohkuma T, Neal B, Jardine MJ, et al. Effect of SGLT2 inhibitors on cardiovascular, renal and safety outcomes in patients with type 2 diabetes mellitus and chronic kidney disease: a systematic review and meta-analysis. Diabetes Obes Metab. 2019;21(5):1237-50.
- Neuen BL, Young T, Heerspink HJL, Neal B, Perkovic V, Billot L, et al. SGLT2 inhibitors for the prevention of kidney failure in patients with type 2 diabetes: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2019;7(11):845-54.
- Zannad F, Ferreira JP, Pocock SJ, Anker SD, Butler J, Filippatos G, et al. SGLT2 inhibitors in patients with heart failure with reduced ejection fraction: a meta-analysis of the EMPEROR-Reduced and DAPA-HF trials. Lancet. 2020;396(10254):819-29.
- Kosiborod M, Cavender MA, Fu AZ, Wilding JP, Khunti K, Holl RW, et al; CVD-REAL Investigators and Study Group. Lower risk of heart failure and death in patients initiated on sodium-glucose cotransporter-2 inhibitors versus other glucose-lowering drugs: the CVD-REAL study (comparative effectiveness of cardiovascular outcomes in new users of sodium-glucose cotransporter-2 inhibitors). Circulation. 2017;136(3):249-59.
- Cavender MA, Norhammar A, Birkeland KI, Jørgensen ME, Wilding JP, Khunti K, et al; CVD-REAL Investigators and Study Group. SGLT-2 inhibitors and cardiovascular risk: an analysis of CVD-REAL. J Am Coll Cardiol. 2018;71(22):2497-506.
- Patorno E, Pawar A, Franklin JM, Najafzadeh M, Déruaz-Luyet A, Brodovicz KG, et al. Empagliflozin and the risk of heart failure hospitalization in routine clinical care. Circulation. 2019;139(25):2822-30.
- Heerspink HJL, Karasik A, Thuresson M, Melzer-Cohen C, Chodick G, Khunti K, et al. Kidney outcomes associated with use of SGLT2 inhibitors in real-world clinical practice (CVD-REAL 3): a multinational observational cohort study. Lancet Diabetes Endocrinol. 2020;8(1):27-35.
- Boehringer Ingelheim. A multicentre international randomized parallel group double-blind placebo-controlled clinical trial of empagliflozin once daily to assess cardio-renal outcomes in patients with chronic KIDNEY Disease [Internet]. clinicaltrials.gov; 2021 [cited 2021 Jun 10]. Report No.: NCT03594110. Available from: https://clinicaltrials.gov/ct2/show/NCT03594110
- Davidson JA. The increasing role of primary care physicians in caring for patients with type 2 diabetes mellitus. Mayo Clin Proc. 2010;85(12 Suppl):S3-4.
- Saudek CD. The role of primary care professionals in managing diabetes. Clin Diabetes. 2002;20(2):65-6.
- Santos Cavaiola T, Kiriakov Y, Reid T. Primary care management of patients with type 2 diabetes: overcoming inertia and advancing therapy with the use of injectables. Clin Ther. 2019;41(2):352-67.
- Patakfalvi L, Brazeau AS, Dasgupta K. Physician experiences with sodium-glucose cotransporter (SGLT2) inhibitors, a new class of medications in type 2 diabetes, and adverse effects. Prim Health Care Res Dev. 2018;20:e50.
- Valensi P, Picard S, Pathak A. Type 2 diabetes: why should diabetologists and cardiologists work more closely together? Diabetes Metab. 2019;45(6):501-4.
|