Abstract
Introduction: Crigler-Najjar syndrome type 2 (CNS type 2) is a rare disorder that causes elevated levels of bilirubin in the blood (nonhemolytic unconjugated hyperbilirubinemia). The main symptom of CNS type 2 is persistent jaundice. It is caused by genetic changes in the UGT1A1 gene and the inheritance is autosomal recessive. Genetic testing of the UGT1A1 gene for mutations is the diagnostic clincher. We report one such rare case. Case report: A 75-year-old male presented with history of right-sided weakness with right-sided facial weakness, MRI brain revealed an infarct in the left side of brain with general physical findings suggestive of icterus. Conclusion: Diagnosing and managing these patients may be challenging. Our aim is to draw attention of the treating physicians towards this disease with the help of this case report.
Keywords: Crigler-Najjar syndrome, isolated indirect hyperbilirubinemia
Crigler-Najjar syndrome (CNS) is an inherited hyperbilirubinemia syndrome, characterized by isolated unconjugated hyperbilirubinemia. Type 2 CNS also known as Arias syndrome, named after the physician who first described it in 1962, Crigler-Najjar type 2 is somewhat more common than type 1. Patients live into adulthood with serum bilirubin levels of 6-25 mg/dL.1 In these patients, mutations in the bilirubin uridine diphosphate-glucuronosyltransferase (UDPGT) gene cause reduction—typically ≤10%—of the enzymatic activity.
Bilirubin UDPGT activity can be induced by the administration of phenobarbital, which can reduce serum bilirubin levels in these patients. Despite marked jaundice, these patients usually survive into adulthood. The prevalence of CNS type 2 is not known but an approximate annual incidence of 1 per million live births has been found in case reports from worldwide for both the types of CNS.2 It is differentiated facilely from its doppelgangers-hemolytic syndrome and Gilbert’s syndrome in which bilirubin levels rarely cross 6 mg/dL.3 In this article, we present a case of CNS type 2 in an adult as it is a rare disorder, and therefore, it is important to draw attention towards such cases.
CASE REPORT
A 75-year-old male presented to the emergency department of our hospital with complaints of right-sided weakness along with right-sided facial weakness. The patient was a known case of type 2 diabetes mellitus and ischemic heart disease. Detailed history revealed that the patient had yellowish discoloration of both the eyes since childhood. The patient was the 7th brother among 8 siblings; all the brothers had a similar history of yellowish discoloration.
On examination, the patient was conscious and oriented to time, place and person. On head to toe examination, the patient had icterus (Fig. 1).
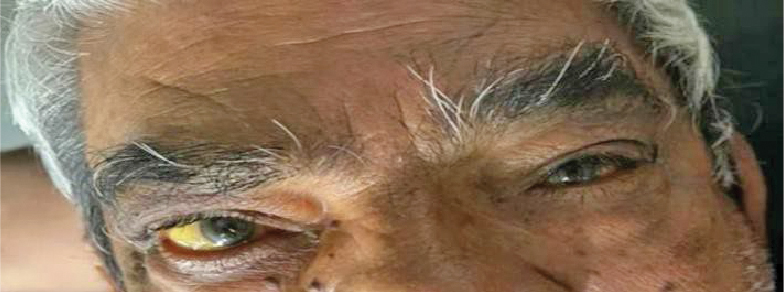
Figure 1. Patient’s eyes showing presence of icterus.
On central nervous system examination, the patient had normal higher mental functions. The right side upper limb had power of 3/5 and the lower limb had power of 3/5, brisk deep tendon reflexes. The right-sided plantar reflex was extensor. On cranial nerve examination, the patient had right-sided upper motor neuron type facial nerve palsy.
An early diagnosis of right-sided hemiparesis with right-sided facial nerve palsy with hyperbilirubinemia was made. The noncontrast computed tomography (NCCT) head obtained initially showed no signs of infarct. The magnetic resonance imaging (MRI) brain on the other hand revealed left-sided infarct.
The biochemical assessment showed total bilirubin levels of 17.6 mg/dL with direct bilirubin levels of 0.2 mg/dL, serum glutamic oxaloacetic transaminase (SGOT) - 27.0 U/L and serum glutamic pyruvic transaminase (SGPT) - 14.4 U/L; other biochemical investigations were within normal limits. There were no markers suggestive of hemolysis. The viral markers for viral hepatitis were negative. The patient was unwilling for liver biopsy. Hence, a provisional diagnosis of CNS type 2 was made after ruling out other causes of isolated hyperbilirubinemia. UGT1A1 gene polymorphism test by PCR fragment analysis revealed Genotype *28/*28 with 2 alleles each with 7 TA repeat (7/7 homozygous) demonstrating severely reduced glucuronidation activity. The other causes of unconjugated hyperbilirubinemia were ruled out.
The patient was treated with antiplatelet agents along with statin therapy, and advised follow-up.
DISCUSSION
As a differential to unconjugated hyperbilirubinemia, CNS is a rare genetic disorder, which is defined by impaired conversion and clearance of bilirubin.
During normal reaction bilirubin produced by the lysis of heme is converted from an unconjugated form to a conjugated form, which dissolves in water and is be excreted out of the body. The patients affected with this syndrome have trouble in converting unconjugated bilirubin into the conjugated form because they lack a specific liver enzyme required in the metabolism of bilirubin. Since there is no conversion of bilirubin, this results in abnormally high levels of unconjugated bilirubin in the blood (unconjugated hyperbilirubinemia).
The defining feature of CNS is a persistent yellowish discoloration of the skin, mucous membranes and sclera (jaundice).
CNS is of two types: CNS type 1, characterized by a nearly complete lack of enzyme activity and severe, potentially fatal symptoms; and CNS type 2, a result of reduced enzyme activity and mild symptoms.
Our patient presented at 75 years of age, but he had developed clinical features of icterus since birth, which is consistent with age group within which this disease usually manifests. He also presented with right-sided hemiparesis and facial nerve palsy. The higher mental functions were normal. No other biochemical abnormalities suggestive of any other hepatobiliary disease were detected. UGT1A1 gene study revealed reduced enzymatic activity. The patient upon detailed history also revealed history of similar illness in all siblings.
The icterus in CNS type 2 persists since early childhood and it is often not associated with kernicterus like features.
The pattern for inheritance for both subtypes of CNS is as autosomal recessive traits and are caused as a result of errors or mutations of the UGT1A1 gene.4
CNS type 2 is usually managed conservatively with avoidance of drugs that displace bilirubin from albumin such as ceftriaxone, furosemide, penicillin, sulfonamides, salicylates. The dose of phenobarbitone preferably used is 60-180 mg/day in single or divided doses.5 The response occurs within 2 to 3 weeks of administration. It is preferred to be given lifelong even though there are minimal symptoms. Clofibrate (2 g/day in divided doses) has also been proved to be equally efficacious. Calcium supplementation has also been found to increase the gut excretion of bilirubin. Plasmapheresis or phototherapy are reserved to deal with a hyperbilirubinemic crisis. Lifelong phototherapy is required rarely.
CONCLUSION
Crigler-Najjar syndrome type 2 is rare genetic disorder of bilirubin metabolism and a rarer cause of jaundice in an adult. A high level of clinical suspicion based on some of its unique features can aid diagnosis. Hence, a patient presenting with asymptomatic indirect hyperbilirubinemia that patient should be evaluated for CNS as a potential differential diagnosis.
Acknowledgment: None.
Funding: No funding was solicited or obtained for this research.
Contributions: SS prepared the draft manuscript under the guidance of SA, SM, CM, MN. Final manuscript was read and approved by all authors for submission.
Ethics Declarations: Ethics approval and consent to participate - Not applicable.
Consent for Publication: Written and informed consent was obtained from patient’s wife as well as father for publication of this case report and any accompanying images which do not include the patient’s photograph.
Conflict of Interests: The authors declare that they have no conflict of interests.
REFERENCES
- Radlovic N. Hereditary hyperbilirubinemias. Srp Arh Celok Lek. 2014;142(3-4):257-60.
- MaruoY, Nakahara S, Yanagi T, Nomura A, Mimura Y, Matsui K, et al. Genotype of UGT1A1 and phenotype correlation between Crigler-Najjar syndrome type II and Gilbert syndrome. J Gastroenterol Hepatol. 2016;31(2):403-8.
- Blueger AF, Krupnikova EZ, Sondore VY, Semushina EP. Study of the etiology and pathogenesis of low grade nonhemolytic unconjugated hyperbilirubinemia (Gilbert’s disease). Acta Hepatogastroenterol (Stuttg). 1977;24(3):140-7.
- Nair KM, Lohse P, Nampoothiri S. Crigler-Najjar syndrome type 2: Novel UGT1A1 mutation. Indian J Hum Genet. 2012;18(2):233-4.
- Ranjan P, Kohli S, Saxena R, Thakur S. Mutation analysis in Crigler-Najjar syndrome type II – case report and literature review. J Clin Exp Hepatol. 2011;1(3):204-6.