Published in IJCP
December 2022
Review Article
Alcohol Use Disorders and Diabetes Mellitus
December 12, 2022 | Priyanka Saha, Yatan Pal Singh Balhara
Internal Medicine
Abstract
Alcohol use disorder is a chronic relapsing brain disorder and is associated with high mortality and morbidity. Chronic alcohol use worsens diabetes and associated diabetes-related complication. Alcohol use, especially over the long-term, can impact the glycemic control in persons with diabetes mellitus. Heavy consumption of alcohol in people with diabetes can lead to worsening of diabetes-related complications like diabetic ketoacidosis, altered lipid metabolism, peripheral neuropathy, sexual dysfunction and cardiovascular disease. This review aims to describe the association between alcohol use and glucose tolerance, effects of alcohol on the pre-existing diabetes; association between alcohol use, diabetes mellitus and diabetes-related complications and interaction of medicines used to treat diabetes with alcohol.
Keywords: Alcohol, alcohol use disorders, diabetes mellitus, insulin, glycemic control
Diabetes mellitus affects 537 million adults globally and a substantial proportion of them are from low- and middle-income countries. In 2021, diabetes accounted for 6.7 million deaths worldwide.1 Alcohol is responsible for around 5% of the global burden of disease. Alcohol contributes a substantial burden socio-economically as well as for the alcohol-attributable diseases. When it comes to middle- and lower-income countries, the mortality and morbidity risks due to alcohol are more in comparison to high-income countries.
Alcohol consumption has been implicated as an independent and modifiable risk factor for the development of diabetes mellitus.2 Several cohort studies have examined the association between alcohol and risk of developing type 2 diabetes mellitus (T2DM). It has been proposed that there is a U-shaped relationship between alcohol consumption and risk of developing diabetes. While moderate alcohol use may reduce the risk of T2DM,3 heavy alcohol use increases the risk.4 In addition, alcohol can have an immediate deleterious effect on diabetes control by worsening hypoglycemia, particularly in individuals using insulin or insulin secretagogues and can also contribute to weight gain.
The current article discusses the association of alcohol intake and glucose tolerance, and the effect of alcohol on blood glucose levels. Furthermore, this article also explores the existing literature on association between alcohol and diabetes mellitus and the pharmacological interventions for alcohol use disorder.
ASSOCIATION BETWEEN ALCOHOL INTAKE AND GLUCOSE TOLERANCE
Following alcohol consumption in individuals with or without diabetes, the glucose disposal rate as well as insulin secretion are increased. Heavy alcohol use leads to beta-cell dysfunction, which predisposes an individual to diabetes mellitus. In individuals with alcohol dependence, appetite regulating peptides like ghrelin and leptin are altered leading to insulin resistance further contributing to the development of diabetes mellitus.5 Common genetic variants have been shown to interact with diabetes and heavy alcohol use.6
There are also conflicting results, where some studies state reduced risk of diabetes with moderate alcohol use, some reported nil and some showed positive association.
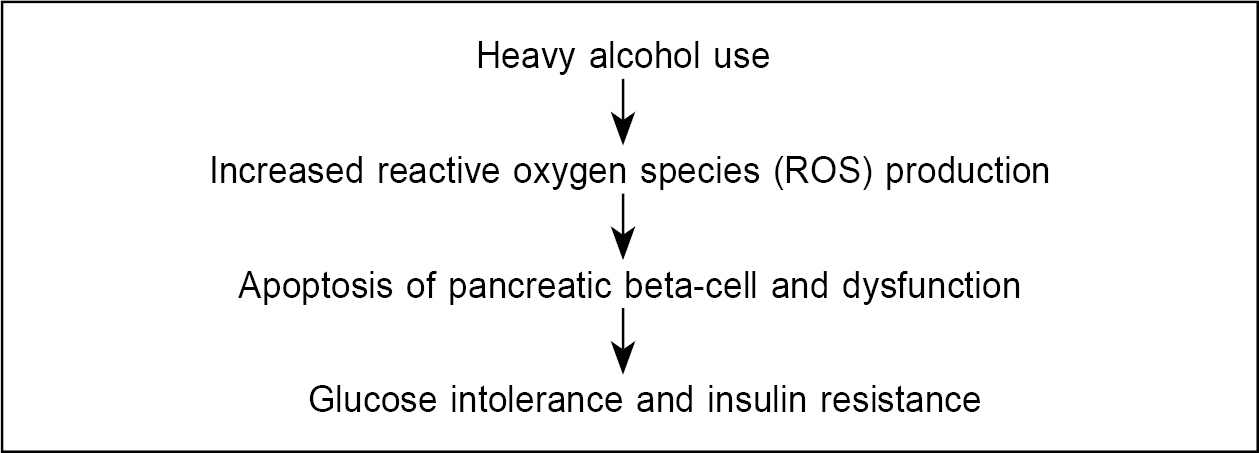
One of the earliest occurrences in glucose intolerance is the production of ROS.5 Animal models have also shown a reduction in glutathione following alcohol administration. Glutathione is an antioxidant and helps in fighting free radical production.7
In a well-fed state, there is a surge in blood glucose level after food intake. In normal individuals, in the absence of diabetes, there is uptake of glucose in the muscle and fat tissues. The existing glucose is converted into glycogen, which acts as a reserve when there is fall in blood glucose level. In type 1 diabetes mellitus (T1DM), since there is no insulin or minimal insulin production, blood glucose level tends to remain high with gradual impairment in both protein and fat metabolism giving rise to serious complications. In T2DM, on the other hand, there is normal to high insulin production and the body initially tries to resist the effect of insulin. In due course, the body cannot produce enough insulin further giving rise to complications.8
Chronic heavy alcohol use leads to decreased insulin secretion and sensitivity. In an individual with pre-existing diabetes, alcohol can worsen fasting as well as postprandial glucose level. Several randomized control trials have looked into the short-term and medium-terms effects of alcohol on blood glucose level in individuals with diabetes.
In the studies (Table 1), which have examined the effect of alcohol use on blood glucose levels, the dose of alcohol has ranged from 12 to 80 g. Majority of the studies had nonsignificant change in the blood glucose level after alcohol consumption. No adverse events of hypoglycemia and withdrawal were reported in any of the studies. Light-to-moderate alcohol consumption has no effect on blood glucose level. Another important factor to note is that the average alcohol intake over a short period of time might not capture the changes in blood glucose level. The pattern of alcohol consumption varies and measurement at a single time frame can give confounding results. Also the effect of heavy alcohol use in glucose level in patients with pre-existing diabetes requires research.
|
Table 1. Effects of Alcohol on Blood Glucose Level in Pre-existing Diabetes
|
|
Author (Year)
|
Type of study
|
Sample size
|
Mean alcohol use
|
Times of glucose measurement
|
Insulin use
|
Result
|
|
Gepner et al (2015)9
|
RCT
|
68
|
16 g of white wine
|
104 weeks
|
11%
|
White wine decreased fasting glucose by 1 mmol/L. Improvement in glycemic control was observed.
|
|
Gepner et al (2015)9
|
RCT
|
73
|
17 g of red wine
|
104 weeks
|
13%
|
No significant decrease in blood glucose level.
|
|
Nakamura et al (2009)10
|
RCT
|
12
|
12 g of white wine
|
26 weeks
|
36%
|
No significant change in blood glucose level.
|
|
Nakamura et al (2009)10
|
RCT
|
12
|
12 g of red wine
|
26 weeks
|
36%
|
No significant change in blood glucose level.
|
|
Kerr et al (2009)11
|
RCT
|
10
|
48-80 g of white wine
|
2 and 4 hours
|
Yes
|
Significant change in blood glucose level after 4 hours.
|
|
Bantle et al (2008)12
|
RCT
|
18
|
24 g of wine
|
2, 4 and 24 hours
|
No
|
No effect on plasma glucose or insulin level.
|
|
Bantle et al (2008)12
|
RCT
|
17
|
18 g of wine
|
4 weeks
|
No
|
No effect on plasma glucose or insulin level.
|
|
Dalgaard et al (2004)13
|
RCT
|
11
|
40 g of ethanol with food
|
0.5, 2, 4 and 24 hours
|
No
|
Alcohol subdues incretin responses in postprandial phase. No significant difference in blood glucose level.
|
|
Koivisto et al (1993)14
|
RCT
|
10
|
61 g (vodka, red wine and cognac)
|
0.5 hours
|
Yes
|
No significant increase in blood glucose level.
|
|
Koivisto et al (1993)14
|
RCT
|
16
|
61 g (vodka, red wine and cognac)
|
0.5, 2, 4 and 24 hours
|
No
|
No effect on postprandial blood glucose level. Serum insulin was higher after 3 hours of food and alcohol intake.
|
Future prospective studies are required to look into the long-term changes associated with alcohol use in pre-existing diabetes.
ASSOCIATION BETWEEN ALCOHOL AND DIABETES MELLITUS
Many studies have explored the role of alcohol as an independent risk factor for diabetes mellitus. As early as 1971, Phillips et al15 stated that a mean alcohol dose of 233-516 mg/dL causes insulin resistance and glucose tolerance. Taking this into account further cross-sectional studies also had similar findings. A meta-analysis by Baliunas et al in 200916 explored the association of alcohol use and diabetes mellitus, where findings of heavy drinkers (>50 g of alcohol/day in women and >60 g of alcohol/day in men) and nondrinkers were similar. No clear conclusion could be figured from the study.
Leggio et al in 2009 looked into the results from the multisite COMBINE study and evaluated the association between blood glucose level, heavy alcohol consumption and craving for alcohol during the treatment process in a sample of 1,324 patients. Baseline blood glucose level was found to have a positive association with percentage of heavy drinking days during treatment suggesting a role of blood glucose in heavy alcohol use.17
A 12-year follow-up study conducted by Lee et al in 2017, which investigated the association of pattern of alcohol consumption and risk of T2DM reported that heavy drinking pattern (>30 g/day) increased the risk of incident diabetes, whereas with light or moderate drinking, the risk was reduced.18
A 12-year follow-up study by Jang et al in 2019, which aimed to determine whether longitudinal association between genetic variants of GCK (glucokinase) or INSR (insulin receptor) in heavy alcohol users was associated with the risk of developing diabetes concluded that the risk of diabetes was increased in chronic heavy alcohol users who had the C allele of GCK. Chronic heavy alcohol consumers who had INSR haplotype negative also were at a higher risk of developing diabetes mellitus.6
ROLE OF ALCOHOL IN DIABETES-RELATED COMPLICATIONS
A systematic review was conducted in 2004 which aimed to look into the effect of alcohol use in incidence, management and complications of diabetes mellitus. Thirty-two studies met the inclusion criteria and affirmed that compared to moderate alcohol use, heavy alcohol consumption was associated with 43% increased risk of developing diabetes mellitus. Two experimental studies looked into the effect of alcohol into diabetic medication-related compilations and found that chlorpropamide (sulfonylurea) was associated with reduced ethanol elimination.19
Alcohol can worsen the complications associated with diabetes mellitus and the mechanisms by which it does so areas described below:
- Diabetic ketoacidosis: Although ketoacidosis is more common in people with T1DM as they completely lack insulin, nevertheless heavy alcohol use can cause ketoacidosis in a person who is not a known diabetic as well. On prolonged heavy alcohol consumption, an individual usually does not consume food and develops low blood glucose levels and can also reduce gluconeogenesis. However, some may have increased levels as in absence of insulin there is less glucose uptake in the tissues. Two important factors resulting in ketoacidosis are lack of insulin and increased glucagon levels.8
- Altered lipid metabolism: Individuals with diabetes are prone to develop dyslipidemia. Initial change in liver pathology following daily alcohol use is fatty liver and heavy alcohol use further leads to steatosis, which sensitizes the liver for further injury.20 Some of the alterations in lipid metabolism seen with alcohol use are increased triglyceride (TG) level, decreased low-density lipoprotein (LDL) and elevated high-density lipoprotein (HDL). A study by Shimomura et al in 2013 investigated the role of alcohol and lipid parameters in 1,477 diabetic individuals and classified their alcohol use into light, moderate and heavy drinkers. Results showed alcohol intake had an inverse relation with high TG/HDL cholesterol ratio in individuals with light and moderate alcohol use, whereas in heavy drinkers the ratio was higher.21 Polymorphism of alcohol dehydrogenase, aldehyde dehydrogenase, genes related to lipid metabolism and apolipoprotein E can lead to altered lipid metabolism in individual with diabetes mellitus and alcohol use.22,23
- Peripheral neuropathy: Clinical presentation of peripheral neuropathy can range from asymptomatic to symptoms such as tingling and numbness, burning sensation and pain, which can be debilitating and is common amongst individuals with diabetes and alcohol use. Diabetic peripheral neuropathy affects small C fibers and to some extent Adelta fibers, whereas in alcoholic neuropathy large fibers are involved, which result from thiamine deficiency.24 Alcohol and diabetes can amplify each other’s effect in causing peripheral neuropathy. A study conducted in 1980 looked into the effect of alcohol intake in 541 individuals with diabetes experiencing symptomatic peripheral neuropathy. In this sample, 15% were heavy drinkers and 7% had frank alcohol use disorder and it was found that symptomatic peripheral neuropathy was much higher among the heavy drinkers.25
- Cardiovascular disease: Chronic heavy alcohol use is associated with hypertension, increased risk of hemorrhagic strokes, cardiomyopathy, heart failure and arrhythmia.26 The relationship between alcohol in individuals with diabetes and acute coronary syndrome has been described as a J-shaped curve where the risk is lowest among light drinkers (<12 g/day) and highest amongst moderate to heavy drinkers (12-24 g and >24 g/day).27 The probable mechanisms proposed were increased TG level and decrease in HDL leading to cardiovascular problems.
- Sexual dysfunction: Mechanisms underlying erectile dysfunction in diabetes mellitus and alcohol are multifactorial and can be vascular, neurogenic and hormonal. Diabetic neuropathy per se worsens the autonomic and somatic nerve processes, which play a role in erection. Low testosterone level has been associated with diabetes mellitus and chronic alcohol use. A study in Japan investigating the pattern of alcohol use causing erectile dysfunction in individuals with T2DM reported a 43% prevalence of erectile dysfunction. Weekly consumption of alcohol <60 g in patients with T2DM was associated with lower erectile dysfunction suggesting an inverse relationship with frequency of alcohol consumption and erectile dysfunction.28
DRUG INTERACTIONS – ALCOHOL USE DISORDER AND DIABETES MELLITUS
The US Food and Drug Administration (FDA) has approved naltrexone, acamprosate and disulfiram for the treatment of alcohol use disorder.29 Other non-FDA approved medications like baclofen, topiramate, gabapentin and nalmefene have also been used to treat alcohol use disorder (Table 2).
|
Table 2. Medications for Alcohol Use Disorder
|
|
Medicines
|
Dosage
|
Adverse effects
|
|
Naltrexone
Injectable naltrexone
|
50 mg/day
FDA approved injectable naltrexone 380 mg/month intramuscularly
|
Nausea, vomiting, decreased appetite, abdominal pain (unsafe in patients with liver disease)
|
|
Acamprosate
|
1998 mg/day orally in 3 divided doses
|
GI upset, diarrhea (safe in patients with liver disease)
|
|
Disulfiram
|
250-500 mg/day
|
Drowsiness, metallic taste, peripheral neuropathy, hepatitis, psychosis, optic neuritis, confusional state
|
|
Baclofen
|
30-80 mg in 3 divided doses
Starting from 5 mg 3 times a day and then 10 mg 3 times a day followed by 20 mg 3 to 4 times a day. Titration of dose to be done in 3 to 7 days till treatment goal is achieved. Can be increased up to 180 mg.
|
Drowsiness, headache, confusion
|
|
Topiramate
|
75-300 mg/day in 2 divided doses
|
Paresthesia, difficulty in attention and concentration, pruritus, anorexia
|
|
Gabapentin
|
600-1800 mg/day in 3 divided doses
|
Dizziness, peripheral edema, gait disorder
|
|
Nalmefene
|
5-80 mg/day in once daily or twice daily dosing
|
Nausea, vomiting, headache
|
There can be both pharmacodynamic as well as pharmacokinetic drug interactions of antidiabetic medications with alcohol. Where kinetic interactions occur at the level of metabolism or absorption of the drug, pharmacodynamic interactions primarily occur at the receptor or tissue level. Table 3 describes the interactions of medications used for treatment of diabetes with alcohol.
|
Table 3. Interaction of Medicines Used to Treat Diabetes with Alcohol
|
|
Medicine
|
Mechanism
|
Studies
|
|
Chlorpropamide (sulfonylurea)
|
Inhibits aldehyde dehydrogenase in the brain and liver.
Can cause disulfiram-like reaction (flushing, nausea, vomiting, sweating) if taken along with alcohol.
|
Ohlin et al (1982)30
|
|
Glyburide
|
Can cause disulfiram-like reaction if taken along with alcohol.
|
Johnson & Seneviratne (2014)31
|
|
Tolbutamide
|
Increased metabolism of tolbutamide.
Can cause disulfiram-like reaction if taken along with alcohol.
|
Carulli et al (1971)32; Kater et al (1969)33
|
|
Tolazamide
|
Can cause disulfiram-like reaction if taken along with alcohol.
|
Jones (2004)34
|
|
Glipizide
|
Alcohol delays the absorption and elimination of gliclazide.
|
Johnson & Seneviratne (2014)31
|
|
Metformin
|
Alcohol increases effect of metformin on lactate metabolism.
|
Schaffalitzky de Muckadell et al (1979)35;
Dubas & Johnson (1981)36
|
|
Troglitazone
|
Worsening of liver function when simultaneously taken.
|
Johnson & Seneviratne (2014)31
|
|
Insulin
|
Alcohol potentiates the action of insulin by lowering the glucose level.
|
Johnson & Seneviratne (2014)31
|
FUTURE CONSIDERATIONS
Co-occurrence of alcohol use (including alcohol use disorders) and diabetes is a significant clinical and public health issue. The effect of heavy alcohol use in glucose level in patients with pre-existing diabetes needs more research. There are gaps in literature about anticraving agents for alcohol use disorder and medications used for diabetes mellitus. More studies are required to know about the course and outcome, profile of patients and quality of life in patients with diabetes and alcohol use disorder to have a better understanding. Indian studies about this are minimal and need further attention.
REFERENCES
- Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119.
- Kao WH, Puddey IB, Boland LL, Watson RL, Brancati FL. Alcohol consumption and the risk of type 2 diabetes mellitus: atherosclerosis risk in communities study. Am J Epidemiol. 2001;154(8):748-57.
- Knott C, Bell S, Britton A. Alcohol consumption and the risk of type 2 diabetes: a systematic review and dose-response meta-analysis of more than 1.9 million individuals from 38 observational studies. Diabetes Care. 2015;38(9):1804-12.
- Wei M, Gibbons LW, Mitchell TL, Kampert JB, Blair SN. Alcohol intake and incidence of type 2 diabetes in men. Diabetes Care. 2000;23(1):18-22.
- Kim SJ, Kim DJ. The relationship between chronic alcohol use and type 2 diabetes mellitus: new insights into mechanisms of appetite-regulating peptides. In: Glucose Tolerance. 2012. pp. 101-22. https://doi.org/10.5772/51795
- Jang HB, Go MJ, Park SI, Lee HJ, Cho SB. Chronic heavy alcohol consumption influences the association between genetic variants of GCK or INSR and the development of diabetes in men: a 12-year follow-up study. Sci Rep. 2019;9(1):20029.
- Kiechl S, Willeit J, Poewe W, Egger G, Oberhollenzer F, Muggeo M, et al. Insulin sensitivity and regular alcohol consumption: large, prospective, cross sectional population study (Bruneck study). BMJ. 1996;313(7064):1040-4.
- Emanuele NV, Swade TF, Emanuele MA. Consequences of alcohol use in diabetics. Alcohol Health Res World. 1998;22(3):211-9.
- Gepner Y, Golan R, Harman-Boehm I, Henkin Y, Schwarzfuchs D, Shelef I, et al. Effects of initiating moderate alcohol intake on cardiometabolic risk in adults with type 2 diabetes: a 2-year randomized, controlled trial. Ann Intern Med. 2015;163(8):569-79.
- Nakamura T, Fujiwara N, Sugaya T, Ueda Y, Koide H. Effect of red wine on urinary protein, 8-hydroxydeoxyguanosine, and liver-type fatty acid-binding protein excretion in patients with diabetic nephropathy. Metabolism. 2009;58(8):1185-90.
- Kerr D, Penfold S, Zouwail S, Thomas P, Begley J. The influence of liberal alcohol consumption on glucose metabolism in patients with type 1 diabetes: a pilot study. QJM. 2009;102(3):169-74.
- Bantle AE, Thomas W, Bantle JP. Metabolic effects of alcohol in the form of wine in persons with type 2 diabetes mellitus. Metabolism. 2008;57(2):241-5.
- Dalgaard M, Thomsen C, Rasmussen BM, Holst JJ, Hermansen K. Ethanol with a mixed meal decreases the incretin levels early postprandially and increases postprandial lipemia in type 2 diabetic patients. Metabolism. 2004;53(1):77-83.
- Koivisto VA, Tulokas S, Toivonen M, Haapa E, Pelkonen R. Alcohol with a meal has no adverse effects on postprandial glucose homeostasis in diabetic patients. Diabetes Care. 1993;16(12):1612-4.
- Phillips GB, Safrit HF. Alcoholic diabetes. Induction of glucose intolerance with alcohol. JAMA. 1971;217(11):1513-9.
- Baliunas DO, Taylor BJ, Irving H, Roerecke M, Patra J, Mohapatra S, et al. Alcohol as a risk factor for type 2 diabetes: a systematic review and meta-analysis. Diabetes Care. 2009;32(11):2123-32.
- Leggio L, Ray LA, Kenna GA, Swift RM. Blood glucose level, alcohol heavy drinking, and alcohol craving during treatment for alcohol dependence: results from the Combined Pharmacotherapies and Behavioral Interventions for Alcohol Dependence (COMBINE) Study. Alcohol Clin Exp Res. 2009;33(9):1539-44.
- Lee DY, Yoo MG, Kim HJ, Jang HB, Kim JH, Lee HJ, et al. Association between alcohol consumption pattern and the incidence risk of type 2 diabetes in Korean men: a 12-years follow-up study. Sci Rep. 2017;7(1):7322.
- Howard AA, Arnsten JH, Gourevitch MN. Effect of alcohol consumption on diabetes mellitus: a systematic review. Ann Intern Med. 2004;140(3):211-9.
- You M, Arteel GE. Effect of ethanol on lipid metabolism. J Hepatol. 2019;70(2):237-48.
- Shimomura T, Wakabayashi I. Inverse associations between light-to-moderate alcohol intake and lipid-related indices in patients with diabetes. Cardiovasc Diabetol. 2013;12:104.
- Chaudhary R, Likidlilid A, Peerapatdit T, Tresukosol D, Srisuma S, Ratanamaneechat S, et al. Apolipoprotein E gene polymorphism: effects on plasma lipids and risk of type 2 diabetes and coronary artery disease. Cardiovasc Diabetol. 2012;11:36.
- Yin RX, Wu DF, Miao L, Aung LH, Cao XL, Yan TT, et al. Several genetic polymorphisms interact with overweight/obesity to influence serum lipid levels. Cardiovasc Diabetol. 2012;11(1):123.
- Zeng L, Alongkronrusmee D, van Rijn RM. An integrated perspective on diabetic, alcoholic, and drug-induced neuropathy, etiology, and treatment in the US. J Pain Res. 2017;10:219-28.
- McCulloch DK, Campbell IW, Prescott RJ, Clarke BF. Effect of alcohol intake on symptomatic peripheral neuropathy in diabetic men. Diabetes Care. 1980;3(2):245-7.
- Klatsky AL. Alcohol, cardiovascular diseases and diabetes mellitus. Pharmacol Res. 2007;55(3):237-47.
- Pitsavos C, Makrilakis K, Panagiotakos DB, Chrysohoou C, Ioannidis I, Dimosthenopoulos C, et al. The J-shape effect of alcohol intake on the risk of developing acute coronary syndromes in diabetic subjects: the CARDIO2000 II Study. Diabet Med. 2005;22(3):243-8.
- Furukawa S, Sakai T, Niiya T, Miyaoka H, Miyake T, Yamamoto S, et al. Alcohol consumption and prevalence of erectile dysfunction in Japanese patients with type 2 diabetes mellitus: Baseline data from the Dogo Study. Alcohol. 2016;55:17-22.
- Kranzler HR, Soyka M. Diagnosis and pharmacotherapy of alcohol use disorder: a review. JAMA. 2018;320(8):815-24.
- Ohlin H, Jerntorp P, Bergström B, Almér LO. Chlorpropamide-alcohol flushing, aldehyde dehydrogenase activity, and diabetic complications. Br Med J (Clin Res Ed). 1982;285(6345):838-40.
- Johnson BA, Seneviratne C. Alcohol-medical drug interactions. Handb Clin Neurol. 2014;125:543-59.
- Carulli N, Manenti F, Gallo M, Salvioli GF. Alcohol-drugs interaction in man: alcohol and tolbutamide. Eur J Clin Invest. 1971;1(6):421-4.
- Kater RM, Tobon F, Iber FL. Increased rate of tolbutamide metabolism in alcoholic patients. JAMA. 1969;207(2):363-5.
- Jones AW. Alcohol and drug interactions. In: Mozayani A, Raymon LP (Eds.). Handbook of Drug Interactions. Totowa, NJ: Forensic Science and Medicine. Humana Press; 2004. pp. 395-462. https://doi.org/10.1007/978-1-59259-654-6_12
- Schaffalitzky de Muckadell OB, Mortensen H, Lyngsøe J. Metabolic effects of glucocorticoid and ethanol administration in phenformin- and metformin-treated obese diabetics. Acta Med Scand. 1979;206(4):269-73.
- Dubas TC, Johnson WJ. Metformin-induced lactic acidosis: potentiation by ethanol. Res Commun Chem Pathol Pharmacol. 1981;33(1):21-31.
|