Abstract
Strategies to improve medication safety focused on acute care settings. Twenty-six studies and descriptions of quality improvement projects were identified. Strategies used to focus on recommendations to prevent medication errors at various stages, from a nationwide voluntary organization to improve safety of patients and empower education system of nurses and other health care providers in safe practices in health care system and vast growing technology.
Keywords: Medication errors, health care delivery, lack of communication, monitoring side effects of drugs, adverse drug reactions, sentinel events, high-risk and alert medications, strategies to reduce medication errors and legal implications
“Success is not final, failure is not fatal: it is the courage to continue that counts.” —Winston Churchill
Medication errors produce a variety of problems for patients, ranging from minor discomfort to substantial morbidity that may prolong hospitalization or lead to death. The 1999 IOM (Institute of Medicine) report implicates medication errors, at least in part, as a direct cause of up to 98,000 patients death annually. Drug errors associated with morbidity and mortality increase inpatient health care costs by an estimated $4700 per hospital admission, or approximately $2.8 million annually for a 700-bed teaching hospital. In addition, time spent by the health care team tracking errors, such as missed doses, can have an effect on time available for direct patient care.
Medication safety is a significant issue in hospitals and throughout health care. Great improvements are needed, and hospitals are making great efforts to reduce errors and increase this aspect of patient safety. Effective leadership and appropriateness of intervention are associated with successful change implementation. Health care professionals play a vital role in improving the quality of care and also in monitoring the quality assurance of patients in health-care settings. Examining the root cause analysis of events, to promote personnel training and communication barriers for corrective action of health care professionals to deliver quality of care to clients. Therefore adding new technology, revising policies and procedures, and providing more education have often been the approaches taken to reduce medication errors.
Need and Relevance of Study
In the Harvard Medical Practice Study, Leape and colleagues examined more than 30,000 hospital discharges selected at random from 51 hospitals in the State of New York in 1984. The researchers found that 3.7% of hospitalizations involved adverse events that prolonged hospital stay or were manifested as a new disability at the time of discharge. About one in four of these adverse events were judged to be attributable to negligence, and 58% were judged to be preventable.
James Reason (1995), a leading author in error management believed people generally do not act in isolation, but that their behavior is influenced by circumstances. He maintained that the likelihood of an unsafe act being committed is heavily influenced by the nature of the task and by the local workplace conditions. Examples include, increasing staffing and decreasing workload, software enhancement or modification, eliminating or reducing distractions, checklists and clinical or critical pathways, eliminate look-alike and sound-alike’s, read back and enhanced documentation and communication. Moreover, there are medication errors that require necessary interventions to sustain life.
Optimization of the medication process can be obtained by adopting various strategies such as medication standardization, clinical pathway/critical pathway, electronic physician order entry system or computerized physician order entry (CPOE) system, barcode technology, electronic medication administration record (EMAR), medication reconciliation (updating current medications prescribed for the patients from admission till discharge).
Objectives
- To assess the pre- and post-test level of knowledge regarding safe medication administration process in experimental and control group of nurses to enhance quality monitor to improve patient care among nurses.
- To evaluate the effectiveness of teaching standardized protocol by comparing the pre- and post-test level of knowledge regarding safe medication process in experimental and control group of nurses to enhance quality monitor to improve patient care among nurses.
- To find out the difference between pre- and post-test level of knowledge regarding safe medication process in experimental and control group of nurses to enhance quality monitor to improve patient care among nurses.
Review of Literature
A literature review is an organized written presentation of what has been published on a topic by scholars. Burns and Groove (2004). The review of literature for this study is presented under the following headings:
- Literature related to medication administration errors among nurses
- Literature related to rates and types of medication administration errors
- Literature related to knowledge on medication administration process among nurses
- Literature related to technology and medication errors among nurses
- Literature related to medication errors and prevention strategies for nurses.
Literature Related to Medication Administration Errors among Nurses
Oliveira et al (2016) systematically conducted a literature review by utilizing the databases: MEDLINE, CINAHL, LILACS, SciELO, BDENF and Cochrane from studies in English, Portuguese or Spanish, published by 2015. Of 594 potential studies, 8 comprised the final sample of the review. The Nursing Activities Score (NAS; 37.5%) and the Therapeutic Intervention Scoring System (TISS; 37.5%) were the instruments most frequently used for assessing nursing workload. Six studies (75.0%) identified the influence of work overload in events of infection, PU (pressure ulcer) and medication errors. This study identifies evidences of the influence of nursing workload on the occurrence of adverse events (AE) in adult patients admitted to the intensive care unit (ICU). Thus, it concludes that the nursing workload of patients in the ICU influenced the occurrence of AE, and nurses must monitor this variable daily to ensure proper sizing of staff and safety of care by prevention of medication errors.
Literature Related to Rates and Types of Medication Administration Errors
A randomized controlled trials (RCTs) and controlled trials (CTs) reporting rates of medication administration errors (MAEs) or related adverse drug events between an intervention group and a comparator group was conducted by Keers et al (2014). Risk ratios (RRs, with 95% confidence intervals [CIs]) were used to examine the effect of an intervention. Ten electronic databases were searched between 1985 and November 2013. Six RCTs and 7 CTs were included. Types of interventions clustered around four main themes: medication use technology (n = 4); nurse education and training (n = 3); changing practice in anesthesia (n = 2) and ward system changes (n = 4). Reductions in MAE rates were reported by 5 studies; these included automated drug dispensing (RR 0.72, 95% CI 0.53-1.00), CPOE (RR 0.51, 95% 0.40-0.66), barcode-assisted medication administration with electronic administration records (RR 0.71, 95% CI 0.53-0.95), nursing education/training using simulation (RR 0.17, 95% CI 0.08-0.38) and clinical pharmacist-led training (RR 0.76, 95% CI 0.67-0.87). Increased or equivocal outcome rates were found for the remaining studies. Weaknesses in the internal or external validity were apparent for most included studies. There is a need to identify effective interventions to minimize the threat posed by MAEs. The study concludes with review and critically appraise interventions designed to reduce MAEs in the hospital setting. There is emerging evidence of the impact of specific interventions to reduce MAEs in hospitals, which warrant further investigation using rigorous and standardized study designs. Theory-driven efforts to understand the underlying causes of MAEs may lead to more effective interventions in the future.
Literature Related to Knowledge on Medication Administration Process among Nurses
Pirinen et al (2015), conducted a study to describe the different stages of Medication Administration Process (MAP) from the registered nurses (RNs’) perspective. A qualitative descriptive research design, with a purposive sample involving thematic interviews of 20 RNs and questions to them in a paper form, was conducted in two medical units. Data were analyzed by using deductive content analysis. The results revealed that RNs confront numerous problems such as equivocal prescriptions, problems with information technology (IT), unavailability or incompatibility of the medicines, a substantial amount of generic substitutions and changing medicine brands. Disruptions and distraction run through each stage of the MAP, excluding prescribing. The RNs desire support in all stages of the MAP. There are areas to improve in each stage of the MAP from the RNs perspective. Real-time and ubiquitous documentation, along with software including the data and knowledge required in medication management, is needed.
Literature Related to Technology and Medication Errors among Nurses
A total of 2,603 articles were initially identified by Hutton et al (2017) and 10 studies, which used prospective before-and-after study design, were fully reviewed in this article. A systematic search of databases was performed from 1998 to December 2016. Studies measuring the effect of bar-coding technology on medication errors were included in a full-text review. Studies with the outcomes other than medication errors such as efficiency or workarounds were excluded. The results of this review show that bar-coding technology may reduce medication errors in hospital settings, particularly on preventing targeted wrong dose, wrong drug, wrong patient, unauthorized drug and wrong route errors. However, few studies have addressed the impact of bar-coding technology with strong prospective methodologies and the research, which has been conducted from both in-pharmacy and bedside implementations.
Literature Related to Medication Errors and Prevention Strategies for Nurses
An cross-sectional descriptive study was conducted by Gorgich et al (2016), to investigate the causes of medication errors and strategies to prevention of them from nurses and nursing student viewpoint. This cross-sectional descriptive study was conducted on 327 nursing staff of Khatam-al-Anbia Hospital and 62 intern nursing students in nursing and midwifery school of Zahedan, Iran, enrolled through the availability sampling in 2015. The data were collected by the valid and reliable questionnaire. To analyze the data, descriptive statistics, t-test and analysis of variance (ANOVA) were applied by use of SPSS software version 16. The results showed that the most common causes of medication errors in nursing were tiredness due to increased workload (97.8%), and in nursing students it was drug calculation (77.4%).
The most important way for prevention in nurses and nursing student’s opinion, was reducing the work pressure by increasing the personnel, proportional to the number and condition of patients and also creating a unit for medication calculation. Also, there was a significant relationship between the type of ward and the mean of medication errors in two groups. Based on the results, it was recommended that nurse-managers resolve the human resources problem, provide workshops and in-service education about preparing medications, side effects of drugs and pharmacological knowledge. Using electronic medications cards is a measure, which would reduce medications errors.
Methodology and Procedures
Research Design
- Research design: Experimental research design-Quasi (pre- and post-test design).
- Research setting: Tertiary care hospital, Chennai.
- Sampling technique: Probability systematic random sampling technique.
- Target population: The target population comprised of all nurses who satisfied the inclusion criteria.
- Accessible population: Comprised of nurses who satisfied the inclusion criteria at a tertiary care hospital, Chennai.
- Sample size: Fifty (25 in experimental and 25 in control) registered nurses/midwives at tertiary care hospital, Chennai.
Description of the research tool
Tool consisted of 3 sections
- Section I – Demographic data: It included the baseline information about the nurses.
- Section II – Structured questionnaire to assess the level of knowledge regarding safe medication administration process (SMAP)*. The score was interpreted as follows:
Scoring key
- Adequate – ≥75%
- Moderately adequate – 50-75%
- Inadequate – <50%
- The scoring key was graded into adequate knowledge, moderately adequate knowledge and inadequate knowledge on percentage basis.
- Section III – Practice observation checklist to assess the enteral route on SMAP*, by using standardized protocol.
Ethical Considerations
Prior permission was obtained from concerned management of hospital. Confidentiality of the information was maintained.
Method of data collection: Observation method.
Plan for data analysis: Descriptive and inferential statistics method.
Analysis and Findings
As per the data most of the nurses were aged between 20 to 29 years (84%, 100%) group, has female (84%, 100%), graduate nurses (64%, 60%) working in general wards (32%, 36%), with years of experience (56%, 36%), employed permanently (56%, 44%) belongs to nuclear family (76%, 72%) in experimental and control group, respectively.
Major Findings
- With regard to knowledge, a significant percentage of nurses had inadequate knowledge (60%, 80%), moderately adequate (40%, 20%) in pre-test (Fig. 1), whereas after teaching standardized protocol on SMAP 100% in experimental and 96% in control group had adequate knowledge; 4% in moderately adequate in post-test and none of them had inadequate knowledge (Fig. 2).
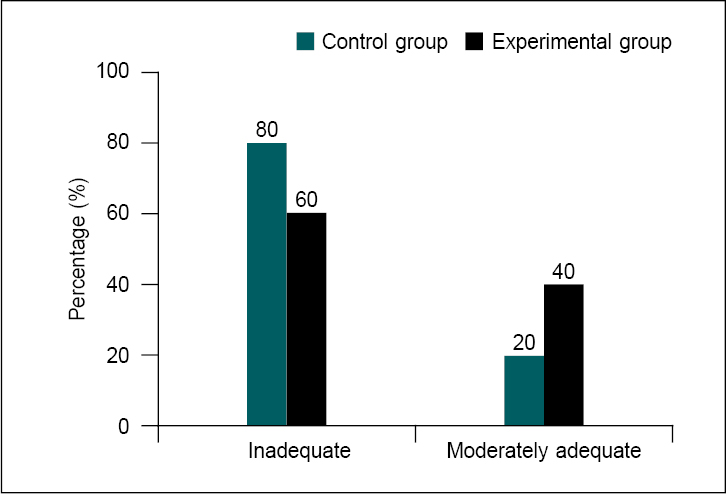
Figure 1. Percentage distribution of level of knowledge pre-test scores on SMAP in experimental and control group during medication process.
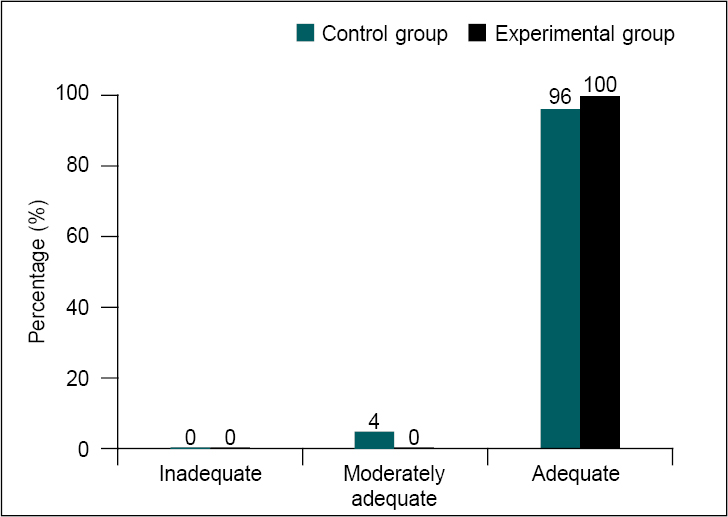
Figure 2. Percentage distribution of level of knowledge post-test scores on SMAP in experimental and control group during medication process.
- With regard to the mean (M) and standard deviation (SD) for the pre-test scores of level knowledge on teaching standardized protocol on SMAP (M = 11.16, SD = 2.528), (M = 10.48, SD = 2.023) showed no significant difference at p > 0.05. On the other hand, after receiving knowledge the mean and SD (M = 23.60, SD = 0.866), (M = 22.84, SD = 1.028) of post-test scores were adequate knowledge when compared with pre-test scores (Fig. 3). The difference was found to be statistically significant at p < 0.01 in experimental and control group of nurses, respectively.
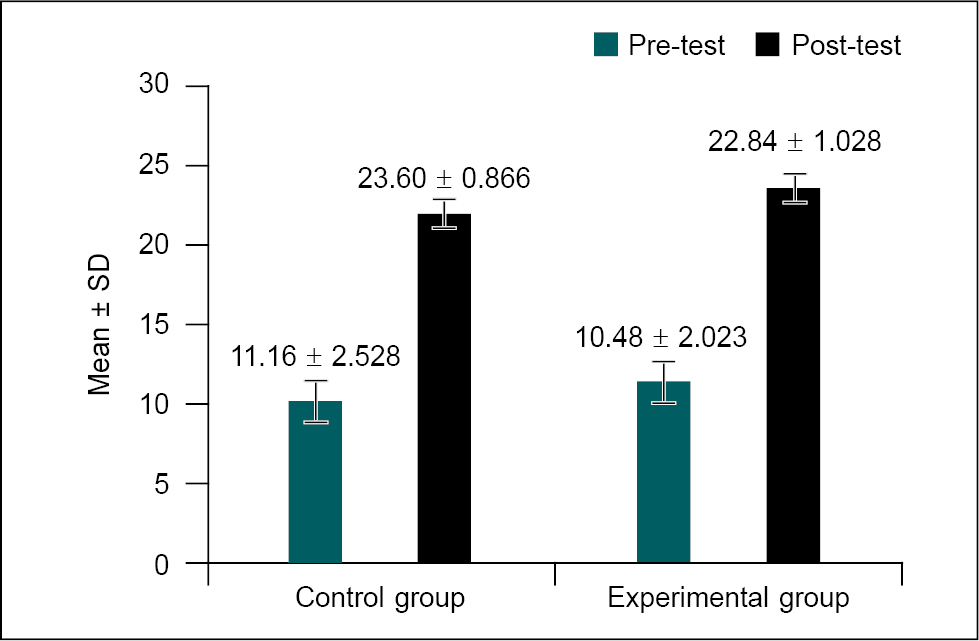
Figure 3. Comparison of mean and SD on pre- and post-test level of knowledge scores on SMAP in experimental and control group of nurses during medication process.
With regard to the mean and SD for the enteral route of medication administration in first post-test observation scores on SMAP (M = 33.7, SD = 0.723), (M = 18.84, SD = 0.374) among nurses was significant at p < 0.01. On the other hand, the enteral route of medication administration in second post-test observation scores (M = 35.56, SD = 0.712), (M = 18.84, SD = 0.374) was statistically significant at p < 0.001 in experimental and control group of nurses; the difference was found statistically significant at p < 0.001, respectively.
Association Findings
These findings reveal that age, gender, educational qualification, area of clinical experience, occupation and type of family were influencing the level of knowledge on SMAP among nurses, which led them to face challenges in health care delivery system (HCDS). Many researchers have recommended by increasing pharmacological knowledge of nurses as a strategy to reduce serious of medication compliance and adverse reaction of drugs. Therefore, nurses are required to update their knowledge about medicines, especially newer drugs. Obviously, it is absolutely impossible to eliminate all medication compliance. However, the role of nursing administrators in reducing and preventing these errors is vital. Reporting medication errors is an ethical duty to maximize the benefits of patient care. It can thus improve patient safety and health. Therefore, managers should have a positive attitude toward the reporting of medication compliance by nurses. Intervention and prevention programs should primarily focus on this type of medication error. More than 75% of nurses strongly agree that continuous education and up-to-date information of pharmacology are necessary to avoid medication errors.
Enhanced communication skills and better interactions among members of the health care team and the patients’ are essential. Reducing medication compliance is an ongoing process of quality improvement. Thus, faculty systems must be redesigned and seamless, computerized integrated medication delivery must be inculcated by health care professionals for adequate training to use such technological advances.
Implications
Nursing Practice
Therefore, it is suggested to train nurses and hospital administrators on facilitators and barriers of error reporting in order to enhance patient safety. Effective prevention of these type of errors depends on the presence of a well-organized reporting system which is able to set targets for costs, quality of information, responsiveness, employee satisfaction and degree of innovation to establish drug distribution system, in respect of quality and cost-effectiveness and represents the best and most cost-effective way of preventing medication errors. Thus, the researchers intend to develop a protocol as prevention strategy for reduction of medication compliance in order to define the differences in quality and cost-effectiveness to enhance the quality improvement among nurses.
Nursing Education
Nursing students can be altruistic and optimistic if they are molded from the beginning. Almost all the nurses follow written guidelines for administering medication. Potential problems were identified in documenting side effects/adverse reactions of medications, storage of medications, student self-administration practices and appropriate authorization of nonprescription drug use. Faculty might consider curriculum revisions that incorporate safety medication use throughout nursing courses. Educational programs to raise awareness and reduce hospital MAEs in children have been delivered to doctors, nurses and graduating students.
Nursing Administration
The role of nursing administrators in reducing and preventing these errors is vital. Although most medication compliance issues can be minor and may not harm the patients, they need more supervision and planning. Nurses involved in a hospital administration should conduct regular skill training programs to empower the novice nurses with three domains (cognitive, conative and affect).
Nursing Research
Many researchers have recommended increasing pharmacological knowledge of nurses as a strategy to reduce serious medication errors. Preparing future generations of nursing professionals with a positive career will be a unique challenge. The Joint Commission International (JCI) advocates the pursuit of continuous improvement in decreasing medication errors so as to enhance patient safety.
Recommendations
- A similar study can be conducted on a large sample to generalize the findings.
- The study can be replicated in different settings.
- A different (exploratory/prospective) study design can be conducted to evaluate awareness about medication errors amongst health care personnel in various hospital settings.
Conclusion
Nurses are most involved in safe medication administration process, although they provide a vital function in detecting and preventing errors that occurred in the prescribing, transcribing, dispensing and administration stages. Research addressing the complex process of medication use in hospitals is urgently needed and requires a new approach to produce valid knowledge from studies done in this field to equip nurses with updated knowledge and skills so as enhance continuous quality improvement to deliver optimum standardized health care services to patients.
Suggested Reading
- Oliveira AC, Garcia PC, Nogueira LS. Nursing workload and occurrence of adverse events in intensive care: a systematic review. Rev Esc Enferm USP. 2016;50(4):683-94.
- Hutton K, Ding Q, Wellman G. The effects of bar-coding technology on medication errors: a systematic literature review. 2021;17(3):e192-e206.
- Keers RN, Williams SD, Cooke J, Walsh T, Ashcroft DM. Impact of interventions designed to reduce medication administration errors in hospitals: a systematic review. Drug Saf. 2014;37(5):317-32.
- Gorgich EA, Barfroshan S, Ghoreishi G, Yaghoobi M. Investigating the causes of medication errors and strategies to prevention of them from nurses and nursing student viewpoint. Glob J Health Sci. 2016;8(8):54448.
- Pirinen H, Kauhanen L, Danielsson-Ojala R, Lilius J, Tuominen I, Díaz Rodríguez N, et al. Registered nurses’ experiences with the medication administration process. Advances in Nursing. 2015;2015:941589.
- Stolic S. Educational strategies aimed at improving student nurse’s medication calculation skills: a review of the research literature. Nurse Educ Pract. 2014;14(5):491-503.
- Thorell A, MacCormick AD, Awad S, Reynolds N, Roulin D, Demartines N, et al. Guidelines for perioperative care in bariatric surgery: Enhanced Recovery After Surgery (ERAS) Society recommendations. World J Surg. 2016;40(9):2065-83.
- Ehsani SR, Cheraghi MA, Nejati A, Salari A, Esmaeilpoor AH, Nejad EM. Medication errors of nurses in the emergency department. J Med Ethics Hist Med. 2013;6:11.
- Bayazidi S, Zarezadeh Y, Zamanzadeh V, Parvan K. Medication error reporting rate and its barriers and facilitators among nurses. J Caring Sci. 2012;1(4):231-6.
- Cheragi MA, Manoocheri H, Mohammadnejad E, Ehsani SR. Types and causes of medication errors from nurse’s viewpoint. Iran J Nurs Midwifery Res. 2013;18(3):228-31.
- Carlton G, Blegen MA. Medication-related errors: a literature review of incidence and antecedents. Annu Rev Nurs Res. 2006;24:19-38.
- Brown MM. Managing medication errors by design. Crit Care Nurs Q. 2001;24(3):77-97.
- Hartly GM, Dillon S. An observational study of the prescribing and administration of intravenous during in a general hospital.Int J Pharm Pract. 1998;8:18-45.
- Koohestani HR, Baghcheghi N. Barriers to the reporting of medication administration errors among nursing students.Aust J Adv Nurs. 2010;27(1):66-74.
- O’Shea E. Factors contributing to medication errors: a literature review. J Clin Nurs.1999;8(5):496-504.
- van Doormaal JE, van den Bemt PM, Mol PG, Zaal RJ, Egberts AC, Haaijer-Ruskamp FM, et al. Medication errors: the impact of prescribing and transcribing errors on preventable harm in hospitalised patients. Qual Saf Health Care.2009;18(1):22-7.
- Latter S, Yerrell P, Rycroft-Malone J, Shaw D. Nursing, medication education and the new policy agenda: the evidence base. Int J Nurs Stud.2000;37(6):469-79.
- Benjamin DM. Reducing medication errors and increasing patient safety: case studies in clinical pharmacology. J Clin Pharmacol.2003;43(7):768-83.
- Chedoe I, Molendijk H, Hospes W, Van den Heuvel ER, Taxis K. The effect of a multifaceted educational intervention on medication preparation and administration errors in neonatal intensive care. Arch Dis Child Fetal Neonatal Ed.2012;97(6):F449-55.