Abstract
More than 4 fibroadenomas in a single breast are uncommon. Repeated recurrences of supernumerary fibroadenomas, in multiple numbers, after excision, are extremely rare. The malignant potential of breast fibroadenoma increases significantly in women with complex fibroadenomas, proliferative disease or a family history of breast cancer. Such a condition poses a management dilemma to the surgeon. Prophylactic bilateral mastectomy is controversial, and requires a rigorous assessment of risk benefit ratio and a better assessment of psychosocial impact and ethical issues. More often than not, the patient prefers repeat excision and close surveillance as the most agreeable course of action; the relatively higher risk of malignancy notwithstanding. Repeated excision as new fibroadenomas appear seems to be a feasible option.
Keywords: Fibroadenoma breast, multiple fibroadenoma, recurrent fibroadenoma, supernumerary fibroadenoma
Breast fibroadenoma is a fairly common condition, accounting for nearly 50% of all breast biopsies, and about 75% biopsies in women under 20 years of age.1,2 The malignant potential of breast fibroadenoma is low at 0.125% to 0.02%.3 But, the same risk increases significantly in women with complex fibroadenomas, proliferative disease or a family history of breast cancer.4
Although up to four fibroadenoma in a single breast are not very uncommon,5,6 Haagensen (1986) and Foster et al (1988) in their two different studies found the incidence to be nearly 16% of all fibroadenomas. But, more than that in a single breast is rare.7 It is possible that many such cases remain unreported. Nevertheless, recurrence of supernumerary fibroadenoma seems to be extremely rare.
Both conservative and surgical management of isolated fibroadenoma have their advocates, generally allowing expectant treatment in younger females up to 30 years of age, and more aggressive surgical treatment for patients who are more than 30 years of age.8,9 The question becomes tricky when there are recurrences, or when there is a family history of breast cancer.
We present such a case. The uniqueness of this case lies in the fact that, besides being young and having supernumerary fibroadenomas (6 in 1 breast and 3 in the other), she had repeated recurrences, in multiple numbers after excision, and had a family history of breast cancer.
Case Report
A 21-year-old young girl presented to our surgical clinic with history of multiple lumps in both breasts for the past 3 years. She had similar lumps about 5 years ago, which were removed from her left breast and were reported to be benign. She noticed that the lumps reappeared within 2 years after surgery, but she postponed consulting a doctor presuming them to be benign as earlier. When some of the lumps attained large size, she came in for treatment.
On clinical examination, 6 lumps in the left breast and 3 in the right breast were palpable. Ultrasound and radio mammograms, and fine needle aspiration cytology confirmed the benign nature of these lesions.
The patient’s mother had died of breast cancer at less than 50 years of age, and her maternal grandfather had carcinoma cheek, although he had died of some other cause. Six lumps from the left breast and 3 from the right breast were removed (Fig. 1) and sent for histopathological examination. All were reported to be benign fibroadenomas. The girl refused for BRCA gene mutation assessment, but agreed for a follow-up in case of recurrence.
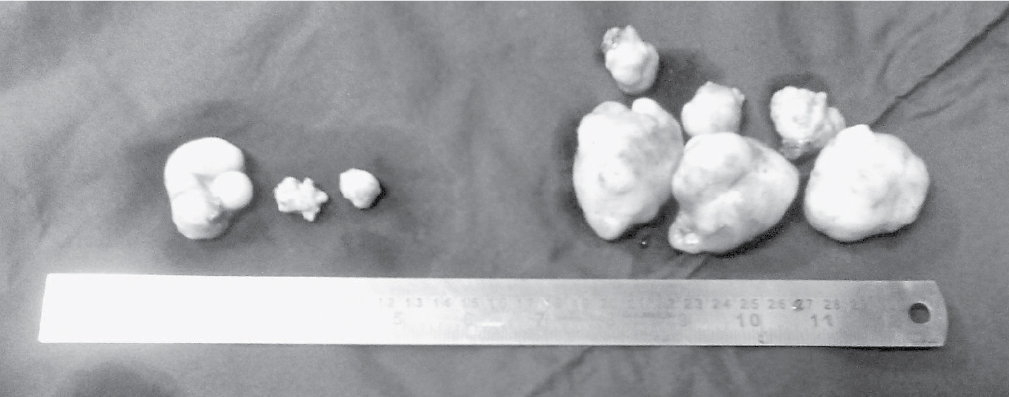
Figure 1. Surgically removed fibroadenomas, 3 from the right breast and 6 from the left breast.
On her last clinical visit on 7th September, 2016, the radio mammography and sonography reports revealed 10 fibroadenomas in the right breast and 5 in the left breast (Fig. 2).
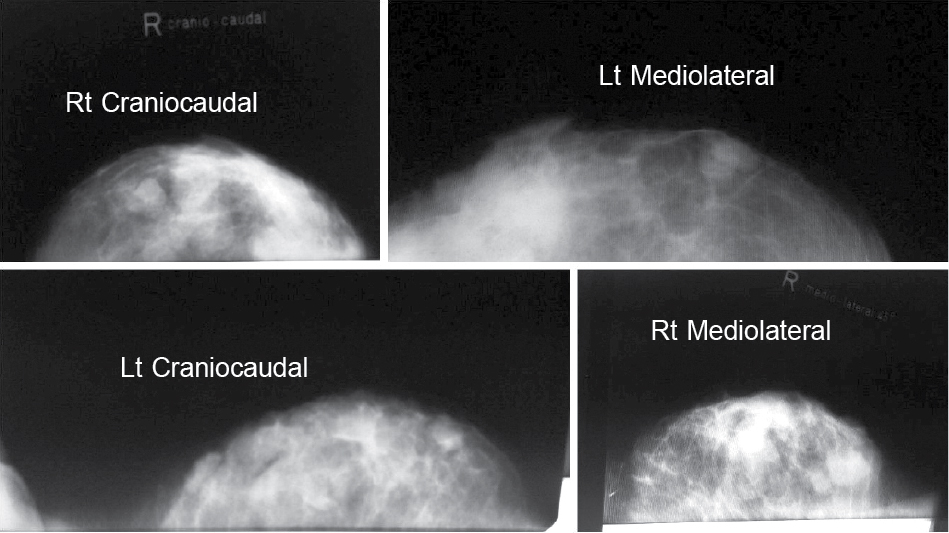
Figure 2. Radio mammography report, at the time of the second recurrence, showing multiple fibroadenomas, 10 in the right breast and 5 in the left breast.
Discussion and Review of Literature
Although breast fibroadenoma is a fairly common disease with a number of 2 to 4 being seen in nearly 16% of all fibroadenomas; finding more than 6 fibroadenomas in a single breast is rare. In 1993, Williamson et al mentioned that they could find only 6 such cases in the literature.7
Fibroadenomas are formed as a result of minor aberrations in the normal process of development and maturation of the breast tissue, and are identical to hyperplastic lobules as shown by various histological studies.10-12 In our case, it was perhaps an ongoing process as evident by such a rapid recurrence in such large numbers. We presume that there were budding fibroadenomas of undetectable size present in both breasts at the time of first and second surgeries, and, may be there would be some present during the subsequent surgeries till this growth period stops at a certain age.
A Mayo Clinic Study (2015) concluded that, although complex, fibroadenomas were more likely to have concomitant high-risk histological features like incomplete involution and proliferative disease without atypia, they alone were not high-risk markers for breast cancer.13
As such, the malignant potential of fibroadenoma breast is extremely low. Zheng et al (2015) could find less than 130 such cases in literature.14 Wu et al (2014) in a detailed analysis of literature mentioned the incidence as 0.125% to 0.02%.3 Pick et al (1984),15 went on to assert that the only importance of fibroadenoma, as far as breast malignancy is concerned, is to contribute to its early detection; and as such they are the parameter independent of the development of cancer in either ipsilateral or contralateral breast.
But, the scenario changes when there is a family history of breast cancer. Dupont et al (1994) in a very well-structured study found that patients having complex fibroadenoma breast and a family history of breast cancer had a relative risk of 3.72 as compared to controls without a family history, of developing cancer.4
Based on the rich data on the natural history of fibroadenoma, (be it single or multiple) and also based on their own experience, Greenberg et al (1998)8 recommended that expectant management for single as well as multiple fibroadenomas is preferable if they are diagnosed before the age of 35 years, and are not increasing in size on a 6-monthly follow-up. In case no regression occurs after the age of 35 years, or if they are increasing in size, they must be excised. Fibroadenoma(s) detected after the age of 35 years can still be observed for 6 to 12 months, but must be excised if they persist beyond that or are increasing in size. In patients with family history of breast cancer, or known changes of complex fibroadenoma, excision biopsy is recommended without delay.
Although the role of BRCA 1/2 gene mutation assessment as a cancer risk predictor is well-established, role of prophylactic mastectomy in high-risk women is still seen with scepticism. Lostumbo et al (2004) in their Cochrane review article, and Rhiem and Schmutzler (2014) in their well-researched article have stressed that a more rigorous assessment of risk benefit ratio and a better assessment of psychosocial impact and ethical issues is required before issuing an undisputable verdict.16,17
Our patient was counseled at length about her increased chances of contracting a malignancy in her breast because her mother had died of breast cancer at an early age of below 50. The girl understood her risk, but absolutely refused to consider a radical surgery like bilateral mastectomy, and, for that matter, even to check her BRCA gene status. We agreed upon a close follow-up and removal of lumps as they appear.
Post the second excision, and on her last clinical visit on 7 September, 2016, she had 10 fibroadenomas in the right breast and 5 in the left breast. She was advised excision of the recurrent fibroadenomas once again.
Conclusion
More than 4 fibroadenomas in a single breast is an extremely rare condition, and repeated recurrence in multiple numbers in such a case is extremely rare.
Early excision irrespective of age must be done, where there is a family history of breast cancer. Prophylactic bilateral mastectomy is a difficult and controversial decision even when there are repeated recurrences in large numbers. It requires a more rigorous assessment of risk benefit ratio and a better assessment of psychosocial impact and ethical issues. More often than not, the patient prefers repeat excision and close surveillance as the most agreeable course of action, the relatively higher risk of malignancy notwithstanding.
References
- Schuerch C 3rd, Rosen PP, Hirota T, Itabashi M, Yamamoto H, Kinne DW, et al. A pathologic study of benign breast diseases in Tokyo and New York. Cancer. 1982;50(9):1899-903.
- Onuigbo WI. Adolescent breast masses in Nigerian Igbos. Am J Surg. 1979;137(3):367-8.
- Wu YT, Chen ST, Chen CJ, Kuo YL, Tseng LM, Chen DR, et al. Breast cancer arising within fibroadenoma: collective analysis of case reports in the literature and hints on treatment policy. World J Surg Oncol. 2014;12:335.
- Dupont WD, Page DL, Parl FF, Vnencak-Jones CL, Plummer WD Jr, Rados MS, et al. Long-term risk of breast cancer in women with fibroadenoma. N Engl J Med. 1994;331(1):10-5.
- Haagensen CD. Diseases of the Breast. 3rd Edition, Philadelphia: WB Saunders; 1986.
- Foster ME, Garrahan N, Williams S. Fibroadenoma of the breast: a clinical and pathological study. J R Coll Surg Edinb. 1988;33(1):16-9.
- Williamson ME, Lyons K, Hughes LE. Multiple fibroadenomas of the breast: a problem of uncertain incidence and management. Ann R Coll Surg Engl. 1993;75(3):161-3.
- Greenberg R, Skornick Y, Kaplan O. Management of breast fibroadenomas. J Gen Intern Med. 1998;13(9):640-5.
- Dixon JM, Dobie V, Lamb J, Walsh JS, Chetty U. Assessment of the acceptability of conservative management of fibroadenoma of the breast. Br J Surg. 1996;83(2):264-5.
- Parks AG. The micro-anatomy of the breast. Ann R Coll Surg Engl.1959;25:235-51.
- Canny PF, Berkowitz GS, Kelsey JL, LiVolsi VA. Fibroadenoma and the use of exogenous hormones. A case-control study. Am J Epidemiol.1988;127(3):454-61.
- Noguchi S, Motomura K, Inaji H, Imaoka S, Koyama H. Clonal analysis of fibroadenoma and phyllodes tumor of the breast. Cancer Res.1993;53(17):4071-4.
- Nassar A, Visscher DW, Degnim AC, Frank RD, Vierkant RA, Frost M, et al. Complex fibroadenoma and breast cancer risk: a Mayo Clinic Benign Breast Disease Cohort Study. Breast Cancer Res Treat. 2015;153(2):397-405.
- Zheng H, Chen J, Wu X, Jin L, Qi C. Bilateral breast cancer with a unilateral carcinoma within a fibroadenoma: A case report. Oncol Lett. 2015;10(3):1513-6.
- Pick PW, Iossifides IA. Occurrence of breast carcinoma within a fibroadenoma. A review. Arch Pathol Lab Med.1984;108(7):590-4.
- Lostumbo L, Carbine N, Wallace J, Ezzo J. Prophylactic mastectomy for the prevention of breast cancer. Cochrane Database Syst Rev.2004;(4):CD002748.
- Rhiem K, Schmutzler R. Impact of prophylactic mastectomy in BRCA1/2 mutation carriers. Breast Care (Basel). 2014;9(6):385-9.