Abstract
Scrub typhus is a common zoonotic disease with high case fatality rate. The clinical presentation of this disease may vary from acute febrile illness, thrombocytopenia, gastrointestinal manifestations, coagulopathy to neurological manifestations. The common neurological manifestations are meningitis and meningoencephalitis, whereas subdural hemorrhage, cerebrovascular accident, i.e., intracerebral hemorrhage, infarct, subarachnoid hemorrhage, etc. are among rare neurological presentations. Scrub typhus-induced neurological disease should be investigated to provide a timely and appropriate diagnosis and to reduce the mortality in complicated scrub typhus infection. Here we report a case of scrub typhus complicated with subdural hemorrhage admitted in our hospital.
Keywords: Scrub typhus, zoonotic, acute febrile illness, neurological, subdural hemorrhage
Scrub typhus also known as bush typhus or tsutsugamushi disease is a zoonotic disease, which spreads to humans through the bite of the trombiculid mite. The trombiculid mites have a four-stage lifecycle: egg, larva, nymph and adult. The infected larva (chiggers) is the only stage that can transmit the disease to humans and other vertebrates.1 The causative organism is Orientia tsutsugamushi which is a Gram-negative intracellular organism. It affects people of all ages including children. Humans are accidental hosts in this zoonotic disease. A billion people are at risk and nearly a million cases are reported every year.2 It is emerging as a notorious disease with mortality rates ranging from <1% to 50% making it a disease with serious public health issues especially in the Asia Pacific region and tsutsugamushi triangle (area of 13 million kilometers) bounded by Pakistan, India and Nepal in the West; Siberia, Japan, China and Korea in the North and Indonesia, Australia, Philippines and the Pacific islands in South.3 Mortality depends on proper antibiotic treatment, status of the individual infected and strain of O. tsutsugamushi encountered.4 This disease is commonly seen in rural areas of India and is common in farmers, geologists and military personnels. Occurrence is influenced by rainfall, with more chiggers attached to the rodents in the wetter months of the year, which may be the reason for clustering of cases during the rainy season as shown by Gurung et al.5
The clinical presentation may range from acute febrile illness, myalgia, arthralgia, thrombocytopenia, acute hepatic dysfunction, acute kidney injury, suffused face, eschar, pneumonitis, acute respiratory distress syndrome, myocarditis, pericarditis to severe neurological manifestations. Among neurologic symptoms are headache, altered sensorium, meningitis, acute disseminated encephalitis, meningoencephalitis, seizure, polyneuritis cranialis and cerebrovascular accident in form infarct, hemorrhage, subdural hemorrhage and cerebral venous thrombosis (CVT).6 Subdural hemorrhage is a rare neurological manifestation reported in scrub typhus patients caused by vasculitis or severe thrombocytopenia. Very few cases had been reported from the state of Rajasthan probably due to less endemicity; however, the prevalence of scrub typhus has increased in Rajasthan since the last few years. Hence, we are reporting a rare case of a young patient of scrub typhus with normal platelet counts with subdural hemorrhage.
CASE REPORT
A 34-year-old male patient, nondiabetic, nonhypertensive admitted in medicine ward in MB Hospital, Udaipur with history of fever with chills, headache, malaise for last 2 days, and altered sensorium for last 1 day. There was no significant past history of seizure, head injury and drug addiction. He had no anemia, cyanosis, icterus, clubbing, edema feet, no hepatosplenomegaly on general physical examination; he was conscious but not oriented to time, place, person. All cranial nerves, deep tendon reflexes were normal with negative Babinski’s sign. Signs of meningeal irritation – neck rigidity, Kernig’s sign were absent. All vital signs were normal (blood pressure was 130/80 mmHg, pulse rate was 96 bpm, respiratory rate was 16 breaths/min), except he was febrile and temperature was 39.6°C (oral).
Auscultation of both lungs revealed normal vesicular breath sounds and no added sounds. Due to the acute febrile illness, a tentative diagnosis of malaria, dengue fever or scrub typhus was suspected. The patient was investigated. The complete blood count (CBC) was normal except for white blood cell (WBC) count, which was raised (24.5 × 103) on day of admission. It came down to normal on day 3 (10.3 × 103). His liver and renal function tests were absolutely normal (urea - 22.6 mg/dL, creatinine - 0.7 mg/dL, total bilirubin - 1.01 mg/dL, serum glutamic-oxaloacetic transaminase [SGOT] - 30 IU/L, serum glutamic-pyruvic transaminase [SGPT] - 25 IU/L, alkaline phosphatase [ALP] - 66 IU/L). Ultrasonography abdomen and chest X-ray were normal. The patient underwent specific investigations for acute febrile illness. Dengue IgG, IgM, NS1 antigen were negative, malaria parasite testing by slide and QBC (Quantitative buffy coat) test was found negative but scrub typhus IgM ELISA (enzyme-linked immunosorbent assay) was positive. Noncontrast computed tomography (NCCT) head was done and showed subdural hemorrhage along the falx. Magnetic resonance imaging (MRI) brain was done and showed early subacute subdural hemorrhage in parafalcine location in bilateral frontal region (Fig. 1). Patient was treated with IV mannitol, IV antiepileptic (phenytoin) along with symptomatic treatment in the form of antibiotic doxycycline, antimalarial, antipyretic and IV fluid, etc. On the third day of admission, improvement in sensorium was seen and the fever subsided. Hence, a diagnosis of scrub typhus with subdural hemorrhage was made.
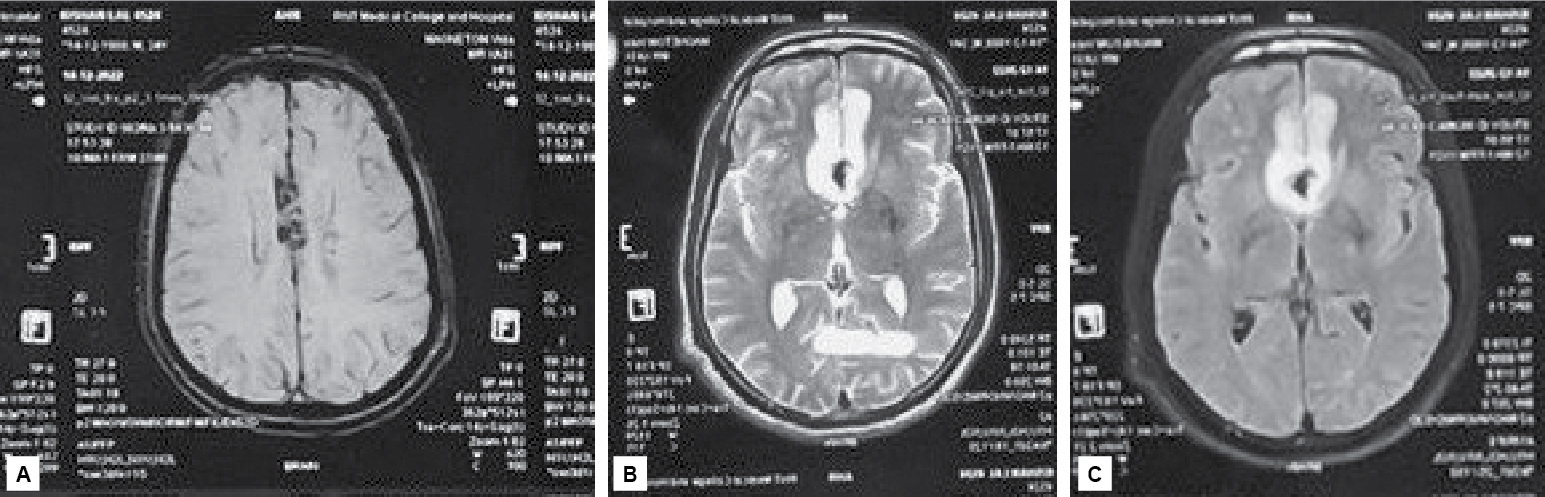
Figure 1. SWI Image shows blooming along parafalcine location (A). T2W (B) and FLAIR (C) images show hyperintensity involving cortical as well as subcortical white matter in bilateral parafalcine frontal location.
DISCUSSION
Scrub typhus is a common mite-borne zoonotic disease distributed mainly in the tsutsugamushi triangle; India is one of the part of this triangle. In India, Himachal Pradesh and Jammu Kashmir are endemic for scrub typhus. There are reports of scrub typhus outbreaks in Himachal Pradesh and Sikkim during 2003-2004 and 2007. But from last few years, this disease has drawn the attention of clinicians in Kerala, Tamil Nadu, West Bengal and Rajasthan also. In Rajasthan, there is a sharp increase in number of cases in the last 5 to 7 years. It is primarily the disease of rural population but since past few years, some cases from urban population also reported. Scrub typhus cases are mainly seen in rainy seasons (July to October) and sporadic cases have been reported throughout the year. The presentation varies from mild self-limiting disease to fatal one leading to death. After an incubation period of 6 to 21 days, onset is characterized by fever, headache, myalgia, cough and gastrointestinal symptoms. Diagnosis is made by serologic assays (indirect fluorescent antibody, indirect immunoperoxidase and enzyme immunoassays). The gold standard is indirect immunofluorescent antibody.7 Molecular detection using polymerase chain reaction (PCR) is possible from skin rash biopsies, lymph node biopsies or ethylenediamine tetraacetic acid blood. GroEL-based real-time PCR assays are more sensitive and give a more quantitative assay.8
Patients are treated predominantly by using antibiotic such as doxycycline/azithromycin/rifampicin/chloramphenicol singly or in combination. Oral/IV doxycycline (100 mg twice daily for 7-15 days), azithromycin (500 mg for 3 days) or chloramphenicol (500 mg 4 times daily for 7-15 days) is usually required. A few patients may present with thrombocytopenia, acute hepatic dysfunction, acute respiratory distress syndrome, acute myocarditis, acute kidney injury, meningitis, encephalitis, meningoencephalitis, subdural hemorrhage and intracerebral hemorrhage, etc. and there is a risk of multiorgan dysfunction. Neurological manifestations are a rare complication in scrub typhus patients and their exact incidences are yet to be documented. Subdural hemorrhage is a rare neurological presentation in these patients and is caused due to extensive vasculitis or due to reduced platelet counts. There are very few cases of subdural hemorrhage reported with normal or mild decrease in the platelet counts and the probable mechanism may be vasculitis (as occurred in our case where platelet count was 469 lakh/mm3 on day first to 362 lakh/mm3 on subsequent days). Scrub typhus exaggerates immune response causing widespread vasculitis and perivasculitis characterized by proliferation of the pathogen in endothelial cells of microvascular system followed by infiltration of monocytes, plasma cells and lymphocytes leading to edema/necrosis in peripheral tissues.9
It therefore manifests as meningitis, encephalitis, acute neuropathy, multiple cranial nerve involvements (2nd, 3rd, 6th, 7th and 8th), CVT, intracerebral infarct and hemorrhage and subdural hemorrhage. A study done by Texier et al10 shows that in patients of scrub typhus, various foci of vasculitis in the form of lymphocytic infiltration of blood vessels are seen.
CONCLUSION
Scrub typhus is now endemic in various parts of India. Subdural hemorrhage is a rare neurological complication of scrub typhus. The mortality rate documented is up to 50% in untreated patients, especially in patients with multiorgan dysfunction. Hence, it is advisable that a patient of acute febrile illness must be evaluated for scrub typhus and patients presenting with fever along with neurological manifestations even with normal platelet counts or mild thrombocytopenia must undergo neuroimaging as soon as possible to diagnose any intracranial hemorrhage, subdural hemorrhage, subarachnoid hemorrhage or infarct and to treat accordingly. Thus, our case report draws the attention of physicians about the possibility of subdural hemorrhage even with normal platelets in association with scrub typhus.
REFERENCES
- Lai CH, Huang CK, Chen YH, Chang LL, Weng HC, Lin JN, et al. Epidemiology of acute q Fever, scrub typhus, and murine typhus, and identification of their clinical characteristics compared to patients with acute febrile illness in Southern Taiwan. J Formos Med Assoc. 2009;108(5):367-76.
- Watt G, Parola P. Scrub typhus and tropical rickettsioses. Curr Opin Infect Dis. 2003;16(5):429-36.
- Walker DH, Dumler JS, et al. Harrison’s Principles of Internal Medicine. 20th Edition, Rickettsial disease: scrub typhus. 2018:20:1303-9
- Kelly DJ, Richards AL, Temenak JJ, Strickman D, Dasch GA. The past and present threat of rickettsial diseases to military medicine and international public health. Clin Infec Dis. 2002;34(Suppl 4):S145-69.
- Gurung S, Pradhan J, Bhutia PY. Outbreak of scrub typhus in the North East Himalayan region-Sikkim: an emerging threat. Indian J Med Microbiol. 2013;31(1):72-4.
- Pai H, Sohn S, Seong Y, Kee S, Chang WH, Choe KW. Central nervous system involvement in patients with scrub typhus. Clin Infect Dis. 1997;24(3):436-40.
- Bozeman FM, Elisberg BL. Serological diagnosis of scrub typhus by indirect immunofluorescence. Proc Soc Exp Biol Med. 1963;112:568-73.
- Paris DH, Aukkanit N, Jenjaroen K, Blacksell SD, Day NP. A highly sensitive quantitative real-time PCR assay based on the groEL gene of contemporary Thai strains of Orientia tsutsugamushi. Clin Microbiol Infect. 2009;15(5):488-95.
- Dumler JS, Siberry GK. Scrub typhus (Orientia tsutsugamushi). (Part XVI. Section 11. Chapter 226) In: Kliegman RM, Behrman Re, Jenson HB, Stanton BF (Eds.). Nelson Textbook of Pediatrics. 18th Edition. Philadelphia: Saunders, Elsevier; 2007. pp. 1295-6.
- Texier P, Rousselot JM, Quillerou D, Aufrant C, Robain D, Foucaud P. Fièvre boutonneuse méditerranéenne. A propos d’un cas mortel chez un nouveau-né [Mediterranean boutonneuse fever. Apropos of a fatal case in a newborn infant]. Arch Fr Pediatr. 1984;41(1):51-3. French.