Abstract
Introduction: Neurological stroke is the most common cause of disability and leaves nearly 65% of survivors with sensory, motor and coordinative disabilities. At present, there are no therapies to prevent long-term neurological deficits after stroke. Many neuroprotective drugs are being tested with the aim to ensure these effects. Preclinical studies have shown a modulatory effect of cerebroprotein hydrolysate on synaptic remodeling and facilitated synaptic transmission. Material and methods: This was a hospital-based, open-label pilot study conducted in a tertiary care hospital of North India. All patients admitted with a diagnosis of stroke both ischemic and hemorrhagic, were included in the study. Patients were randomized into two groups. The test group was given cerebroprotein hydrolysate, along with standard treatment for stroke, whereas the other group was kept on standard treatment for stroke as per the latest guidelines, without cerebroprotein. Results: A total of 50 patients of stroke, admitted in a tertiary care center were included in the study. The mean age of the patients was 65.7 ± 11.86 years. Twenty-six (52%) were males and 24 (48%) were females. Out of the total 50 patients, 23 (46%) had ischemic stroke and 27 (54%) had hemorrhagic stroke. Twenty (40%) had diabetes, 37 (74%) had hypertension, 8 (16%) were known cases of coronary artery disease, 28 (56%) had dyslipidemia, 22 (44%) were smokers, 7 (14%) had a history of ethanol consumption and 13 (26%) were obese. Mean Barthel score at admission was 21.2 ± 11.3 and mean Rankin score at admission was 3.6 ± 1.37. Mean Barthel score at end of treatment was 53.9 ± 28.72 and mean Rankin score at end of treatment was 2.6 ± 1.65. The mean duration of admission was 6.8 ± 3.57 days. Conclusion: The current study highlights the role of cerebroprotein hydrolysate in improving the neurological scores and reducing hospital stay among patients hospitalized with stroke.
Keywords: Barthel score, Rankin score, neuroprotective, neurological deficit
Neurological stroke remains the most common cause of disability and leaves nearly 65% of survivors with sensory, motor and coordinative disabilities.1 At present, there are no therapies to prevent long-term neurological deficits after stroke. Pharmacological interventions in the acute management of stroke aim to restore blood flow to the ischemic tissue in order to minimize brain damage and future complications. Many neuroprotective drugs are being tested with the aim to ensure these effects. Cerebroprotein hydrolysate is a neuropeptide preparation that mimics the action of endogenous neurotrophic factors and protects the brain against the impact of stroke by supporting the cerebral reorganization process.2 Preclinical studies have shown a modulatory effect of porcine brain tissue hydrolysate on synaptic remodeling and facilitated synaptic transmission.3 It has also shown improvement in oligodendrogenesis and neurogenesis.4 Thus, cerebroprotein hydrolysate has shown a beneficial effect on endogenous brain recovery processes in various model systems of stroke and traumatic brain injury.5
In previous studies with neuroprotective agents in stroke patients, there has been a mismatch between preclinical studies and clinical trials, probably due to a failure to activate long-term brain repair processes.6 Stroke causes neuronal damage within gray matter and axonal injury within white matter tracts.7 Cerebroprotein hydrolysate is a mixture of low-molecular-weight neuropeptides derived from purified porcine brain tissue. The ability to penetrate biological membranes and pass through the blood-brain barrier makes cerebroprotein hydrolysate a strong candidate for clinical use in stroke patients. In vivo, cerebroprotein hydrolysate has been demonstrated to improve functional outcomes, promote neurogenesis, reduce neuroinflammation and inhibit free radical formation.8,9
MATERIAL AND METHODS
This was a hospital-based, open-label pilot study conducted in a tertiary care hospital of North India. Fifty patients admitted with a diagnosis of stroke were included in the study. Out of all the stroke patients, 23 suffered from ischemic stroke and 27 from hemorrhagic stroke. Patients were randomized into two groups. A total of 25 patients were randomly assigned to each group. The test group was given cerebroprotein hydrolysate, along with standard treatment for stroke, as per the existing guidelines for ischemic and hemorrhagic stroke, respectively; whereas the other group was kept on standard treatment for stroke, as per the latest guidelines but without cerebroprotein.
The baseline characteristics were recorded and the patients were followed from the day of admission to the day of discharge/death for changes in Rankin and Barthel scores. Improvement in the above-mentioned scores and the duration of stay were taken into account to compare the two groups. Data were analyzed using SPSS software. Continuous variables with normal distribution were expressed as mean ± standard deviation (SD), and the differences were assessed with analysis of variance (ANOVA). Categorical variables were presented as absolute and relative frequencies, and the differences were assessed with Fisher’s test. A ‘p’ value of <0.05 was considered statistically significant. Kendall’s Tau correlation test, McNemar’s test, Paired sample t-test and Wilcoxon signed-rank test were used to compare changes before and after therapies, wherever applicable. A regression model was generated to analyze the effect of cerebroprotein on duration of hospital stay.
RESULTS
A total of 50 patients of stroke, admitted in a tertiary care center were studied. Mean age of the patients was 65.7 ± 11.86 years. Twenty-six (52%) were males and 24 (48%) were females. Out of the total stroke patients, 23 (46%) had ischemic stroke and 27 (54%) had hemorrhagic stroke. Twenty (40%) had diabetes, 37 (74%) had hypertension, 8 (16%) were known cases of coronary artery disease, 28 (56%) had dyslipidemia, 22 (44%) were smokers, 7 (14%) had a history of ethanol consumption and 13 (26%) were obese. Mean Barthel score at admission was 21.2 ± 11.3 and mean Rankin score at admission was 3.6 ± 1.37. Mean Barthel score at end of treatment was 53.9 ± 28.72 and mean Rankin score at end of treatment was 2.6 ± 1.65. The mean duration of admission was 6.8 ± 3.57 days. Table 1 presents the baseline characteristics at admission.
|
Table 1. Baseline Characteristics of Cases and Controls
|
| |
Number (%)
|
|
Males
|
26 (52)
|
|
Ischemic stroke
|
23 (46)
|
|
Hemorrhagic stroke
|
27 (54)
|
|
Diabetes
|
20 (40)
|
|
Hypertension
|
37 (74)
|
|
CAD
|
8 (16)
|
|
Dyslipidemia
|
28 (56)
|
|
Smoking
|
22 (44)
|
|
Alcohol
|
7 (14)
|
|
Obesity
|
13 (26)
|
CAD = Coronary artery disease.
Out of the total 50 patients, 25 (50%) were given daily cerebroprotein injections along with the standard management of stroke as per the guidelines and the remaining 25 (50%) were given only the standard management, without cerebroprotein injections. Barthel scores and Modified Rankin scores were assessed on admission and at discharge.
The differences between Barthel scores on admission and discharge were significant in the two groups with their respective p values (Table 2). The differences between Modified Rankin scores on admission and discharge were significant in the case group but not in control group with their respective p values (Table 2, Figs. 1 and 2).
|
Table 2. Differences in Barthel Scores and Rankin Scores at Admission and Discharge in the Two Groups
|
|
Scores
|
Mean
|
SD
|
P value
|
|
Cases
|
Barthel score at admission
Barthel score at discharge
Rankin score at admission
Rankin score at discharge
|
19.6000
65.4000
3.7600
1.9200
|
24.78743
29.71812
1.20000
1.63095
|
0.004
<0.001
|
|
Controls
|
Barthel score at admission
Barthel score at discharge
Rankin score at admission
Rankin score at discharge
|
22.6667
42.7083
3.5000
3.2917
|
16.90
23.49
1.56
1.428
|
0.04
0.26
|
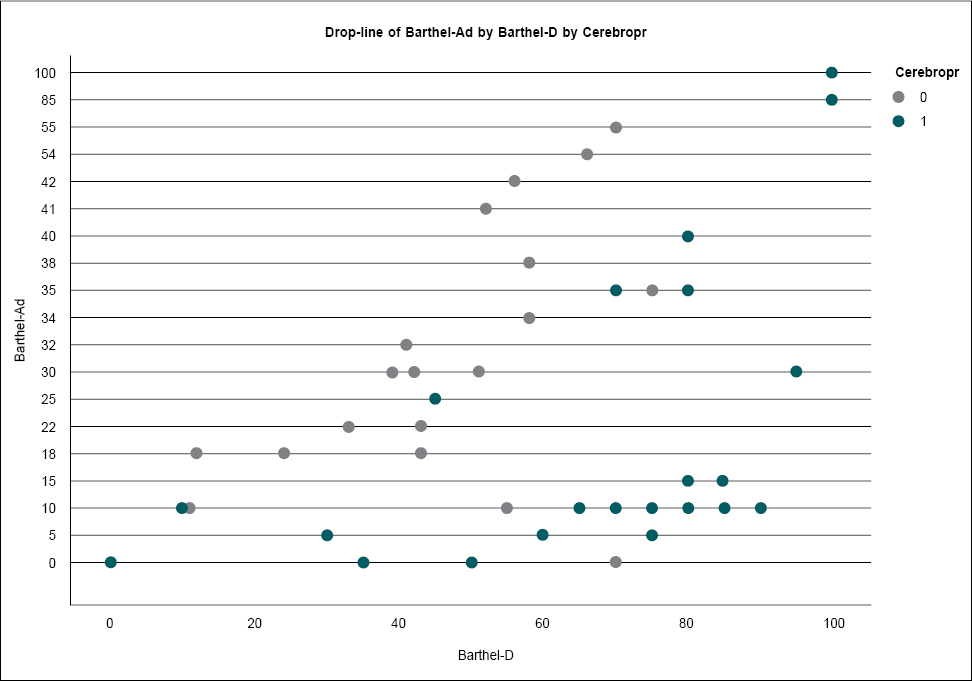
Figure 1. Comparison of changes in Barthel scores on admission and discharge between the two groups.
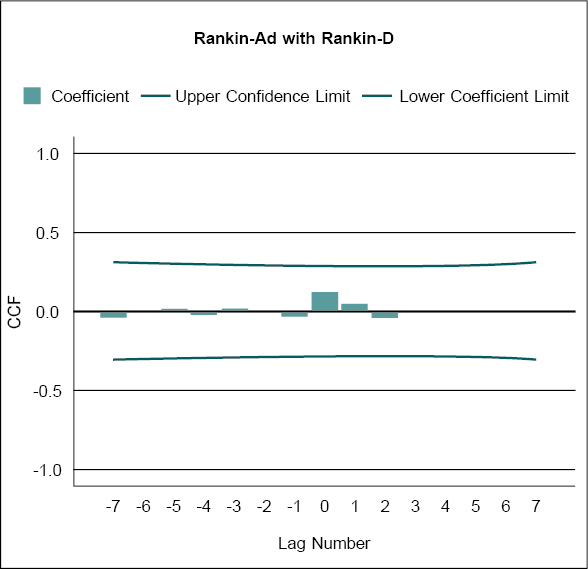
Figure 2. Comparison of changes in Rankin scores on admission and discharge between the two groups.
The average duration of hospital stay in those given cerebroprotein was 4.8 ± 2.11 days; whereas, the average duration of stay in the control group was 7.8 ± 3.89 days (p = 0.02). Figure 3 shows the relationship of duration of hospital stay with cerebroprotein supplementation ascertained using regression plots.
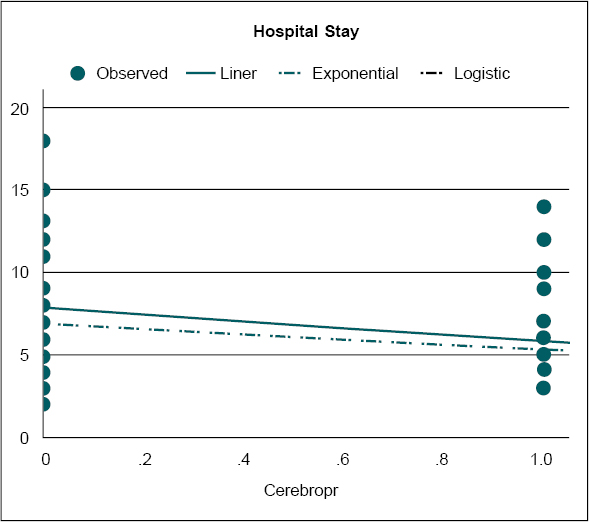
Figure 3. Regression analysis, showing the difference in duration of hospital stays between the two groups.
DISCUSSION
The present study was conducted on 50 stroke patients to compare the improvement in neurological functioning between two groups of patients.
The mean age of the patients in our study was 65.7 ± 11.86 years with 52% males and 48% females. Twenty patients had diabetes, 37 had hypertension, 8 had history of coronary artery disease, 28 had dyslipidemia, 22 were smokers, 7 had history of ethanol consumption and 13 were obese. This is in concert with previous studies on stroke patients. Charan et al have reported a mean age of 55 years in stroke patients.8 In another study by Sridharan et al, the median age of stroke patients was 67 years.10 A recent study conducted in Gujarat by Eapen et al also found that modifiable risk factors such as hypertension (40%), alcoholism (35%) and smoking (28%) are the commonest associations of stroke.11
The efficacy of the treatment was assessed using standardized scales, which showed that the Barthel scores were significantly better (p < 0.01) in all items (personal hygiene, bathing, feeding, toilet, stair climbing, dressing, bowel control, bladder control, ambulation and chair/bed transfer) in the case group. Also, the Modified Rankin Scale showed more improvement (p < 0.01) in the case group, as compared to the control group.
The result of this study showed that in the case group, the mean Barthel score was 19.6000 (± 24.78) and Modified Rankin score was 3.7600 (± 1.2) at the time of admission and the mean Barthel score was 65.4 (± 29.71) and Modified Rankin score was 1.9200 (± 1.63) at the time of discharge. These results were consistent with a similar study conducted by Charan et al on 100 ischemic and hemorrhagic stroke patients, in which two out of four groups received cerebroprotein hydrolysate and in those two groups, Barthel Index score at baseline were 15 and 13 and at the end of 12 weeks were 88 and 84, Modified Rankin score at baseline were 4.64 and 4.80 and at the end of 12 weeks were 2.21 and 2.28, showing that patients receiving cerebroprotein hydrolysate had significant improvement in functional outcomes of patients.8
The differences in the mean Barthel score and mean Modified Rankin score on admission and discharge were significant (p < 0.001) in the two groups in our study. These results were consistent with the similar study conducted by Haffner et al.12
The average duration of hospital stay in the case group was 4.8 ± 2.11 days while in control group was 7.8 ± 3.89 with p value being 0.02, which was significant.
These results suggest that patients receiving cerebroprotein hydrolysate injections along with standard therapy show higher level of improvement in neurological functions as compared to those receiving only standard therapy. Cao et al in their study on mice assessed the long-term effect of cerebroprotein hydrolysate on gray and white matter integrity as well as axonal plasticity in late stage of ischemic stroke.13 They observed an increase in the SMI/MBP ratio after distal middle cerebral artery occlusion (MCAO), which indicates the exacerbation of white matter injury encompassing both axons and myelin in mice; this injury was mitigated by cerebroprotein hydrolysate treatment and hence has role in improvement in sensorimotor functional outcomes in stroke patients.
Cerebroprotein hydrolysate further facilitated the in situ endogenous axonal regeneration and tract-tracing assessment of axons projecting from the contralesional motor cortex in animal models.13 Similar studies conducted in the past have shown that cerebroprotein hydrolysate improves neurological functioning after stroke and plays a key role in post-stroke rehabilitation.14 This may be due to the fact that cerebroprotein hydrolysate is porcine brain tissue derivative containing bioactive substances and free amino acids, which can simulate the effects of neurotropic factors such as brain-derived neurotrophic factor (BDNF), glial cell-derived neurotrophic factor (GDNF), ciliary neurotrophic factor (CNF) and nerve growth factor (NGF).15
Ren et al suggested in their study that cerebroprotein hydrolysate may exert a protective effect by mediating the MEK-ERK-CREB pathway, increasing BDNF expression, and thus improving neurological function and apoptosis in MCAO/reperfusion (MCAO/R) rats and concluded that cerebroprotein hydrolysate may regularly ameliorate the neural function, apoptosis and cerebral infarct volume in MCAO/R rats. It promotes multiple brain remodeling processes including angiogenesis, neurogenesis and axonal regeneration.15
In our study, significant improvement was observed in mean Barthel score in both groups but it was greater in the case group. Significant improvement was seen in modified Rankin score in the case group but no significant improvement was seen in control group. Therefore, we propose an approach combining cerebroprotein hydrolysate with standard therapy for treatment of stroke patients.
Cerebroprotein hydrolysate has not been reported to produce serious side effects. Few side effects like nausea, headache, vertigo, perspiration, confusion, irritability, fever, hallucinations, etc. have been reported. It is contraindicated in hypersensitivity, epilepsy and severe renal impairment. It should be used with caution in pregnant and lactating ladies as the safety profile is still not established.16 Our study was limited by a small sample size. So, further studies with a larger sample size and studies on safety profile of cerebroprotein hydroysate are needed.
CONCLUSION
The current study highlights the role of cerebroprotein hydrolysate in improving the neurological scores and reducing hospital stay among patients admitted with stroke. To the best of our knowledge, this is the first study to take into account both ischemic and hemorrhagic strokesat the same time. The improvement in stroke assessment scores is a confirmation of the in vivo studies, highlighting the role of cerebroprotein in neuroregeneration after stroke.
REFERENCES
- Ovbiagele B, Kautz S, Feng W, Adkins DL. Poststroke outcomes. Stroke Res Treat. 2014;2014:828435.
- Reinprecht I, Gschanes A, Windisch M, Fachbach G. Two peptidergic drugs increase the synaptophysin immunoreactivity in brains of 24-month-old rats. Histochem J. 1999;31(6):395-401.
- Xiong H, Wojtowicz JM, Baskys A. Brain tissue hydrolysate acts on presynaptic adenosine receptors in the rat hippocampus. Can J Physiol Pharmacol. 1995;73(8):1194-7.
- Zhang L, Chopp M, Meier DH, Winter S, Wang L, Szalad A, et al. Sonic hedgehog signaling pathway mediates cerebrolysin-improved neurological function after stroke. Stroke. 2013;44(7):1965-72.
- Tatebayashi Y, Lee MH, Li L, Iqbal K, Grundke-Iqbal I. The dentate gyrus neurogenesis: a therapeutic target for Alzheimer’s disease. Acta Neuropathol. 2003;105(3):225-32.
- Shi L, Rocha M, Leak RK, Zhao J, Bhatia TN, Mu H, et al. A new era for stroke therapy: integrating neurovascular protection with optimal reperfusion. J Cereb Blood Flow Metab. 2018;38(12):2073-91.
- Kinnunen KM, Greenwood R, Powell JH, Leech R, Hawkins PC, Bonnelle V, et al. White matter damage and cognitive impairment after traumatic brain injury. Brain. 2011;134(Pt 2):449-63.
- Charan S, Singh IP, Singh H, Sehgal R, Singh G, Neki NS. A comparative study of citicoline vs cerebroprotein hydrolysate in ischemic and haemorrhagic stroke. Int J Curr Res Med Sci. 2017;3(4):1-6.
- An L, Han X, Li H, Ma Y, Shi L, Xu G, et al. Effects and mechanism of cerebroprotein hydrolysate on learning and memory ability in mice. Genet Mol Res. 2016;15(3).
- Sridharan SE, Unnikrishnan JP, Sukumaran S, Sylaja PN, Nayak SD, Sarma PS, et al. Incidence, types, risk factors, and outcome of stroke in a developing country: the Trivandrum Stroke Registry. Stroke. 2009;40(4):1212-8.
- Eapen RP, Parikh JH, Patel NT. A study of clinical profile and risk factors of cerebrovascular stroke. Guj Med J. 2009;64(2):47-54.
- Haffner Z, Gmeinbauer R, Moessler H. A randomized, double-blind, placebo-controlled trial with cerebrolysin in acute ischemic stroke. Cerebrovasc Dis. 2001;11:76.
- Cao W, Zhang C, Chen R, Wu Q, Xu R, Zhang L, et al. A novel cerebroprotein hydrolysate, CH1, ameliorates chronic focal cerebral ischemia injury by promoting white matter integrity via the Shh/Ptch-1/Gli-1 signaling pathway. Neuropsychiatr Dis Treat. 2020;16:3209-24.
- Oommen A. Cerebroprotein hydrolysate- new paradigm in management of neurological problems. J Neurol Stroke. 2015;2(6):62-5.
- Ren Y, Ma X, Wang T, Cheng B, Ren L, Dong Z, et al. The cerebroprotein hydrolysate-I plays a neuroprotective effect on cerebral ischemic stroke by inhibiting MEK/ERK1/2 signaling pathway in rats. Neuropsychiatr Dis Treat. 2021;17:2199-208.
- Phirke M, Desousa A, Shah N, Sonavane S, Bharati A. The use of cerebroprotein hydrolysate in dementia: a case series of 25 cases seen in a tertiary general hospital. J Geriatr Ment Health. 2014;1:106-9.