Abstract
Background: Recurrent aphthous stomatitis (RAS) is a common ulcerative disease of the oral mucosa, which is difficult to treat. In Ayurveda, several medicinal plants have been evaluated for their anti-inflammatory and antioxidant effects in many oral diseases as an alternative for modern medicines. Method: A study with open-label, non-comparative single-arm design was conducted to evaluate the efficacy of “Stomatab” capsules in improving oral health in 30 subjects with RAS. The secondary objectives were to assess the improvement in oral health and tolerability of the herbal formulation. Subjects were instructed to take one capsule thrice daily after meals for 14 days. Patients were evaluated at three assessment points: screening and baseline (Visit 1, Day 0) with follow-ups done at Visit 2 (Day 5 ± 2) and Visit 3 at the end of the study (Day 14 ± 2). Results: There was a significant reduction in the mean ulcer size from 3.66 ± 1.27 mm (V1) to 0.64 ± 0.78 (V3). The mean number of ulcers reduced from 1.97 ± 0.72 (V1) to 0.90 ± 0.66 (V3). Significant improvement in ulcer-related symptoms of pain (Ruja), burning sensation (Daha) and redness (Raktavarnata) was noted. The total ulcer symptom scores decreased from 7.67 ± 2.38 (V1) to 0.63 ± 0.56 (V3). No side effects were reported by the study participants. Conclusion: These results show that the polyherbal formulation “Stomatab” capsule is safe and effective for the treatment of RAS.
Keywords: Polyherbal, oral mucosa, ulcer size, ulcer symptom score, Jasminum grandiflorum, Mimusops elengi, Ficus religiosa, Red ochre
Recurrent aphthous stomatitis (RAS) is a common ulcerative disease of the oral mucosa.1 These lesions are usually round or oval in shape, with a yellow or grey ground and a surrounding erythematous halo of inflamed mucosa. They can cause significant pain and make eating, speaking and swallowing difficult.2 RAS affects 5% to 25% of the population and is more common in patients aged 10 to 40 years.3 It is a difficult disorder to treat. All treatments aim to reduce the painful symptoms and duration of the ulcers. Although topical or systemic antibacterial agents such as chlorhexidine and other anti-inflammatory, immunomodulatory or symptomatic treatments are used, they are not completely reliable.4 In Ayurveda, several medicinal plants have been evaluated for their anti-inflammatory and antioxidant effects in many oral diseases as an alternative for modern medicines. Therefore, an open-label non-comparative prospective clinical study was conducted to evaluate the efficacy and safety of an Ayurvedic proprietary medicine “Stomatab” capsule containing Jasminum grandiflorum, Mimusops elengi, Ficus religiosa and Red ochre, in human subjects suffering from recurrent oral ulcers or stomatitis.
The primary objective of the study was to evaluate the efficacy of “Stomatab” herbal formulation in improving oral health in subjects susceptible to recurrent canker sores (aphthous ulcers)/stomatitis. The secondary objectives were to assess the improvement in oral health and tolerability of the herbal formulation.
METHODS
A study with an open-label, non-comparative single-arm design was conducted to examine the efficacy and safety of “Stomatab” oral capsule in subjects suffering from mouth ulcer/stomatitis. Potential subjects, aged 18 to 35 years, were recruited from the physicians at the time of their routine examination visit or from the clinical practice of the site investigator.
Patients with oral ulcers on the tongue, cheeks, inside the lips, palate; minor aphthous ulcers numbering 1 to 5; recurrent stomatitis at less than 2 months interval and who were willing to follow the study protocol were included in the study.
Patients with traumatic ulcer, history of cancer (including solid tumors, hematologic malignancies and carcinoma in situ), any neurological (congenital or acquired), vascular or systemic disorder which could affect assessment of efficacy; significant uncontrolled comorbid disease; major aphthous ulcer, herpetiform ulcer were excluded from the study. Patients who had participated in any clinical trial in the past 1 month and those who could not comply with the study protocol were also not included in the study. No concomitant medications were allowed during the course of the study. They prescribed appropriate medication, if they developed any symptom, which was documented.
Patients were evaluated at three assessment points: screening and baseline (Visit 1, Day 0) with follow-ups done at Visit 2 (Day 5 ± 2) and Visit 3 at the end of the study (Day 14 ± 2). Written informed consent was obtained from the participants on the first visit. The vital signs, size and number of ulcers, ulcer symptom scores on 4-point scale and adverse events were recorded during these visits. The study was carried out according to the Declaration of Helsinki, Indian Council of Medical Research (ICMR) ethical guidelines for biomedical research and International Conference on Harmonization (ICH) guidelines for Good Clinical Practice (GCP).
Data were abstracted and presented as a number, percentage, mean and standard deviation (SD). All efficacy and safety variables were summarized using descriptive statistics. Data comparison between baseline and follow-up visits was performed using a paired t-test or one-way analysis of variance (ANOVA), as appropriate and data were expressed as mean, SD, 95% confidence interval (CI) and p-value. Statistical analysis was done using statistical software SPSS 10.0. A p value of 0.05 was considered statistically significant.
RESULTS
A total of 30 subjects were recruited for this study including 9 (30%) females and 21 (70%) males. Subjects were instructed to take one capsule thrice daily after meal for a period of 14 days. All 30 subjects completed the study. The demographic information of the participants is summarized in Table 1.
|
Table 1. Summary of Demographic Data of the Subjects (n = 30)
|
|
Parameters
|
Range
|
Number (%)
|
Mean
|
SD
|
|
Age (year)
|
19-35
|
-
|
25.10
|
5.41
|
|
Male
|
-
|
21 (70%)
|
-
|
-
|
|
Female
|
-
|
9 (30%)
|
-
|
-
|
|
Height (cm)
|
155-175
|
-
|
165.10
|
5.67
|
|
Weight (kg)
|
53.0-67.60
|
-
|
60.08
|
4.84
|
Assessment of Ulcer Size Reduction
The distance between two opposed boundaries of the ulcer edge was measured with a periodontal probe to assess the reduction in mean ulcer size from baseline to the follow-up visits. Results showed a significant reduction in the mean of ulcer size from baseline to the end of the study. Mean changes in ulcer size on days 5 and 14 were found to be statistically significant (p < 0.0001) compared to day 0 (Table 2 and Fig. 1).
|
Table 2. Comparison of Mean Change in Ulcer Size from Day 0 to Different Follow-up Visits (n = 30)
|
|
Parameters
|
Visit (V)
|
Mean score (mean ± SD)
|
Change from V1 (mean ± SD)
|
95% CI of Diff.
|
P value
|
|
Ulcer size (mm)
|
V1
|
3.66 ± 1.27
|
-
|
-
|
<0.0001
|
| |
V2
|
1.90 ± 1.14
|
1.76 ± 0.73
|
1.281-2.245
|
|
| |
V3
|
0.64 ± 0.78
|
3.02 ± 0.99
|
2.535-3.499
|
|
Mean ulcer size at day 0 (V1) was compared with days 5 (V2) and 14 (V3) by one-way ANOVA test. Comparison: V1 vs. V2 and V3.
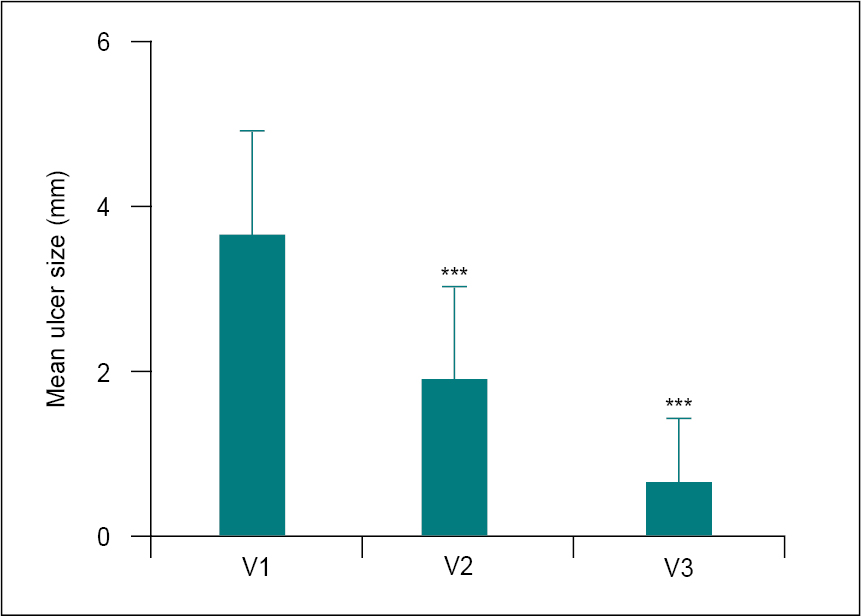
Figure 1. Comparison of mean change in ulcer size from day 0 (V1) to different follow-up visits (n = 30).
Mean of ulcer sizes at V1 was compared with visits V2 and V3 using one-way ANOVA. Comparison: V1 vs. V2 and V3. Significance level ***p < 0.0001.
Assessment for Reduction in Number of Ulcers
There was a significant reduction in the number of ulcers from day 0 to days 5 and 14. Mean changes in the number of ulcers on day 14 was found to be statistically significant (p < 0.0001) compared to day 0 (Table 3 and Fig. 2).
|
Table 3. Comparison of Mean Change in the Number of Ulcers from Day 0 to Different Follow-up Visits (n = 30)
|
|
Parameters
|
Visit (V)
|
Mean score (mean ± SD)
|
Change from V1 (mean ± SD)
|
95% CI of Diff.
|
P value
|
|
Number of ulcer
|
V1
|
1.97 ± 0.72
|
-
|
-
|
-
|
| |
V2
|
1.73 ± 0.69
|
0.23 ± 0.43
|
-0.202-0.669
|
ns
|
| |
V3
|
0.90 ± 0.66
|
1.07 ± 0.58
|
0.631-1.502
|
<0.0001
|
Mean of the number of ulcer at day 0 (V1) was compared with days 5 (V2) and 14 (V3) by one-way ANOVA test. Comparison: V1 vs. V2 and V3.
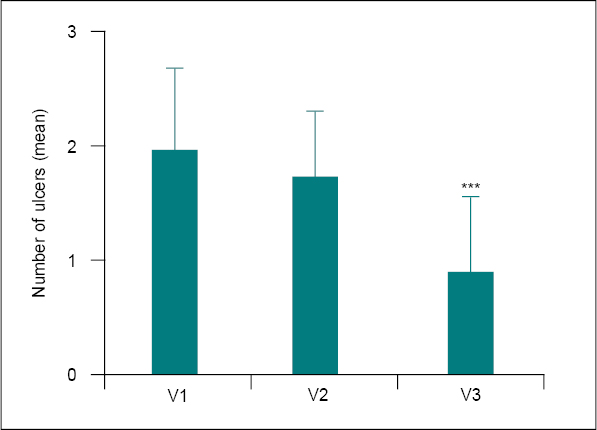
Figure 2. Comparison of mean change in number of ulcers from day 0 (V1) to different follow-up visits (n = 30).
Mean of the number of ulcers at V1 was compared with visits V2 and V3 using one-way ANOVA. Comparison: V1 vs. V2 and V3. Significance level ***p < 0.0001.
Assessment of Ulcer Symptoms
Assessment of the ulcer symptoms such as pain (Ruja), burning sensation (Daha) and redness (Raktavarnata) of the ulcers were assessed on a 4-point scale at all assessment points. All ulcers related symptom scores were significantly (p < 0.001) reduced at days 5 and 14 compared to baseline. The total ulcer symptoms score also significantly reduced from 7.67 ± 2.38 (baseline) to 4.53 ± 1.72 and 0.63 ± 0.56 at days 5 and 14, respectively (Table 4 and Fig. 3).
|
Table 4. Comparison of Mean Change in Ulcer Symptom Scores from Baseline to Different Follow-up Visits (n = 30)
|
|
Parameters
|
Visit (V)
|
Mean score (mean ± SD)
|
Change from V1 (mean ± SD)
|
95% CI of Diff.
|
|
Pain (Ruja)
|
V1
V2
V3
|
2.87 ± 1.17
1.83 ± 1.09
0.57 ± 0.57
|
-
1.03 ± 1.22***
2.30 ± 1.12***
|
-
0.418-1.649
1.684-2.916
|
|
Burning sensation (Daha)
|
V1
V2
V3
|
2.27 ± 0.83
1.37 ± 0.76
0.47 ± 0.51
|
-
0.90 ± 0.88***
1.80 ± 0.76***
|
-
0.450-1.350
1.350-2.250
|
|
Redness (Raktavarnata)
|
V1
V2
V3
|
2.53 ± 0.86
1.33 ± 0.66
0.63 ± 0.56
|
-
1.20 ± 0.76***
1.90 ± 0.71***
|
-
0.756-1.644
1.456-2.344
|
|
Total score
|
V1
V2
V3
|
7.67 ± 2.38
4.53 ± 1.72
0.63 ± 0.56
|
-
3.13 ± 1.48***
7.03 ± 2.11***
|
-
2.046-4.221
5.946-8.121
|
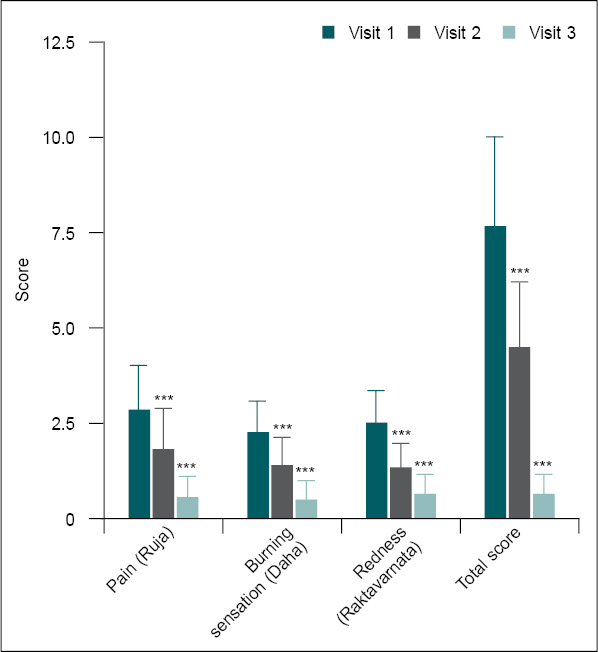
Figure 3. Comparison of mean change in ulcer symptom scores from baseline (V1) to different follow-up visits (n = 30).
Ulcer symptom scores at V1 were compared with follow-up visits (V2 and V3) using one-way ANOVA. Comparison: V1 vs. V2 and V3. Significance level ***p < 0.001.
Safety Assessment
There was no significant difference in vital sign parameters (heart rate and blood pressure) between screening and day 14, and all values were within the normal range (Table 5 and Fig. 4).
|
Table 5. Comparison of Mean Change in Vital Signs from Baseline to Different Follow-up Visits
|
|
Parameters
|
Visit (V)
|
Mean ± SD
(n = 30)
|
Change from V1 (mean ± SD)
|
95% CI of Diff.
|
|
Heart rate (bpm)
|
V1
V2
V3
|
70.27 ± 3.81
71.23 ± 3.41
71.90±3.40
|
-
-0.97 ± 3.29
-1.63±3.12
|
-
-3.202-1.268
-3.868-0.602
|
|
SBP
(mm/Hg)
|
V1
V2
V3
|
113.57 ± 4.90
112.47 ± 5.30
113.33 ± 4.05
|
-
1.10 ± 3.63
0.23 ± 3.59
|
-
-1.910-4.110
-2.776-3.243
|
|
DBP
(mm/Hg)
|
V1
V2
V3
|
77.20 ± 2.07
77.07 ± 1.48
77.03 ± 1.35
|
-
0.13 ± 2.53
0.17 ± 2.46
|
-
-0.917-1.184
-0.884-1.217
|
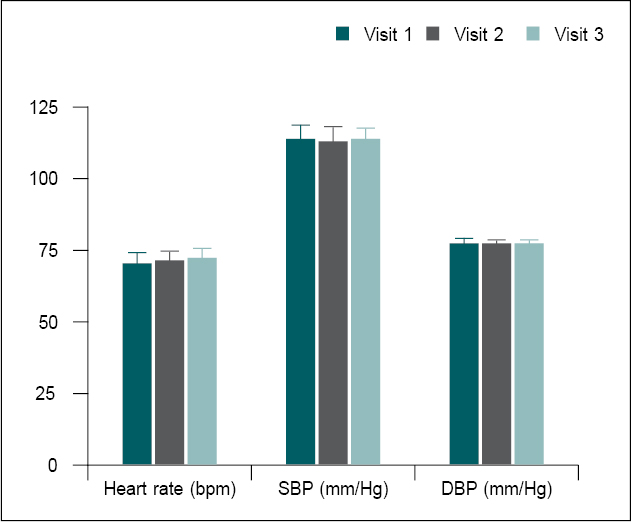
Figure 4. Comparison of mean change in vital signs from baseline to different follow-up visits.
Vital signs data at baseline (V1) were compared to days 5 (V2) and 14 (V3) using the one-way ANOVA test. Comparison: V1 vs. V2 and V3.
No significant difference in the complete blood count (CBC) parameters between screening and day 14, and all values were within the normal range (Table 6 and Fig. 5).
|
Table 6. Comparison of Mean Change in CBC Parameters from Baseline to Day 14
|
|
Parameters
|
Visit (V)
|
Mean ± SD (n = 30)
|
Change from V1 (mean ± SD)
|
95% CI of Diff.
|
P value
|
|
RBC (Million/cumm)
|
V1
V3
|
4.95 ± 0.33
4.93 ± 0.26
|
0.02 ± 0.15
|
-0.036-0.076
|
0.47
|
|
Hb (g/dL)
|
V1
V3
|
14.64 ±1.63
14.61 ± 1.70
|
0.03 ± 0.44
|
-0.133-0.197
|
0.69
|
|
WBC (10^9/L)
|
V1
V3
|
9.53 ± 1.12
9.51 ± 1.02
|
0.01 ± 0.35
|
-0.118-0.142
|
0.85
|
|
Neutrophils (%)
|
V1
V3
|
56.47 ± 1.59
56.03 ± 1.83
|
0.44 ± 2.30
|
-0.418-1.298
|
0.30
|
|
Lymphocytes (%)
|
V1
V3
|
35.48 ± 1.66
35.39 ± 2.0
|
0.09 ± 2.64
|
-0.90-1.073
|
0.86
|
|
Monocytes (%)
|
V1
V3
|
4.58 ± 1.45
5.12 ± 1.88
|
-0.54 ± 2.60
|
-1.511-0.431
|
0.26
|
|
Eosinophils (%)
|
V1
V3
|
2.72 ± 0.75
2.67 ± 0.75
|
0.05 ± 1.03
|
-0.339-0.432
|
0.81
|
|
Basophils (%)
|
V1
V3
|
0.76 ± 0.20
0.74 ± 0.14
|
0.02 ± 0.25
|
-0.076-0.109
|
0.72
|
|
Platelet count
(x1000/cumm)
|
V1
V3
|
306.0 ± 36.64
309.0 ± 33.01
|
-2.73 ± 28.56
|
-13.40-7.929
|
0.60
|
|
ESR (mm 1st hour)
|
V1
V3
|
11.50 ± 4.31
11.53 ± 2.22
|
-0.03 ± 4.88
|
-1.856-1.789
|
0.97
|
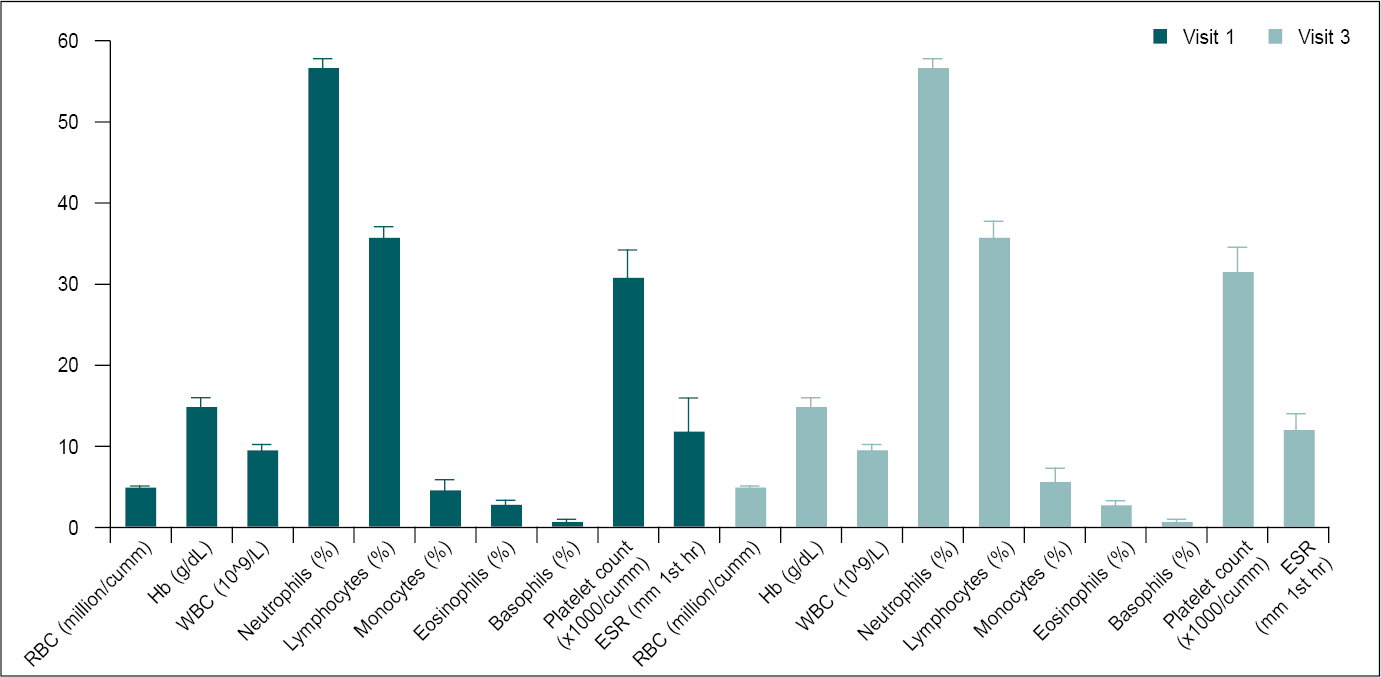
Figure 5. Comparison of mean change in CBP parameters from screening to day 14 (n = 30).
CBP parameters at screening (V1) were compared to day 14 (V3) using paired t-test. Comparison: V1 vs. V3.
Serum levels of blood urea nitrogen (BUN) and creatinine were found to be in the normal range at baseline and day 14 (Table 7 and Fig. 6).
|
Table 7. Comparison of Mean Change in Renal Function Parameters from Baseline to Day 14
|
|
Parameters
|
Visit (V)
|
Mean ± SD
(n = 30)
|
Change from V1 (mean ± SD)
|
95% CI of Diff.
|
P value
|
|
BUN (mg/dL)
|
V1
V3
|
12.71 ± 4.46
13.31 ± 4.25
|
-0.61 ± 5.30
|
-2.584-1.373
|
0.54
|
|
Serum creatinine (mg/dL)
|
V1
V3
|
0.88 ± 0.19
0.84 ± 0.20
|
0.04 ± 0.29
|
-0.068-0.148
|
0.46
|
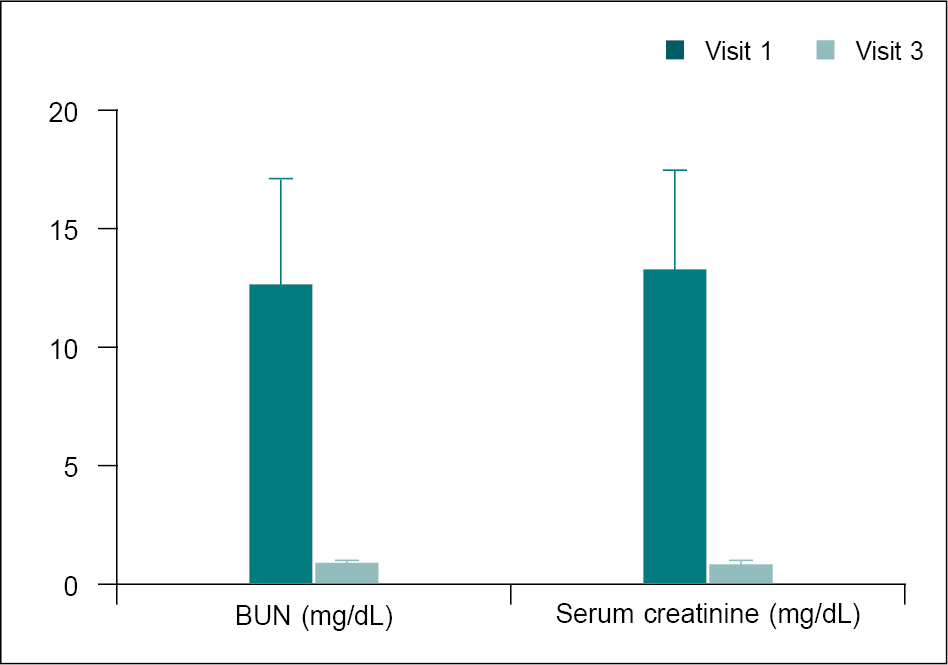
Figure 6. Comparison of mean change in renal function parameters from the baseline to the day 14 (n = 30).
Renal function parameters at baseline (V1) were compared with day 14 (V3) using the paired t-test. Comparison: V1 vs. V3.
Total cholesterol, triglycerides (TG), high-density lipoprotein (HDL), low-density lipoprotein (LDL), very-low-density lipoprotein (VLDL) cholesterol, as well as the Chol:HDL ratio were not remarkably changed at day 14 when compared to baseline. All serum lipid parameters were within the normal range (Table 8 and Fig. 7).
|
Table 8. Comparison of Mean Change in Serum Cholesterol Levels from Baseline to Day 14
|
|
Parameters
|
Visit (V)
|
Mean ± SD
(n = 30)
|
Change from V1 (mean ± SD)
|
95% CI of Diff.
|
P value
|
|
Total cholesterol (mg/dL)
|
V1
V3
|
151.80 ± 16.70
149.60 ± 14.97
|
2.13 ± 19.04
|
-4.983-9.233
|
0.55
|
|
TG (mg/dL)
|
V1
V3
|
121.40 ± 5.30
125.20 ± 5.15
|
-3.80 ± 7.55
|
-6.617-0.976
|
0.01*
|
|
HDL cholesterol (mg/dL)
|
V1
V3
|
67.62 ± 5.87
68.94 ± 4.97
|
-1.32 ± 7.97
|
-4.294-1.656
|
0.37
|
|
LDL cholesterol (mg/dL)
|
V1
V3
|
84.07 ± 7.47
80.29 ± 7.17
|
3.78 ± 8.93
|
0.449-7.119
|
0.03*
|
|
VLDL cholesterol (mg/dL)
|
V1
V3
|
20.38 ± 5.61
19.95 ± 5.17
|
0.43 ± 5.18
|
-1.500-2.366
|
0.65
|
|
Chol:HDL ratio
(mg/dL)
|
V1
V3
|
2.26 ± 90.28
2.18 ± 0.27
|
0.070 ± 0.31
|
0.07
|
0.20
|
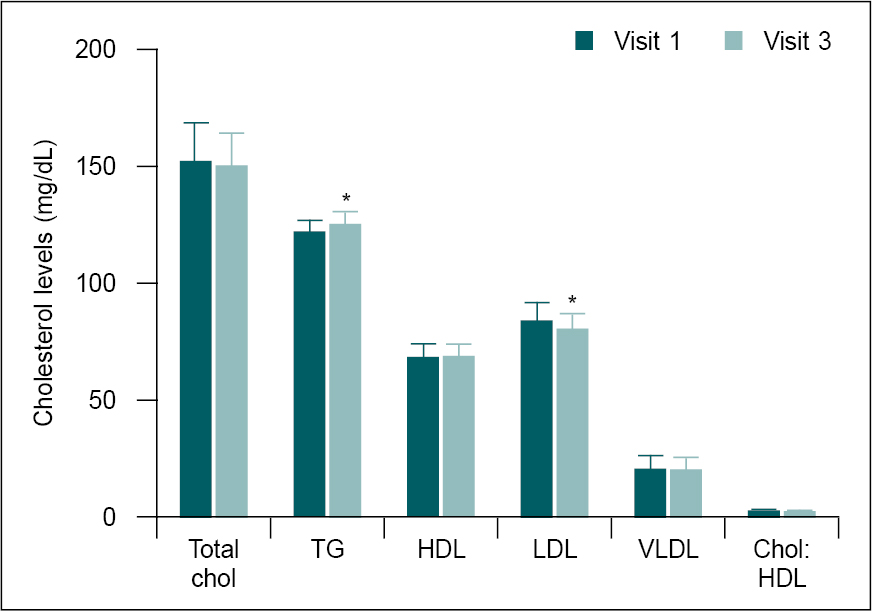
Figure 7. Comparison of mean change in serum cholesterol levels from baseline to day 14 (n = 30).
Serum cholesterol parameters at baseline (V1) were compared with day 14 (V3) using the paired t-test. Comparison: V1 vs. V3. Significance level *p < 0.05.
The liver function parameters including serum levels of serum glutamic-oxaloacetic transaminase (SGOT) and serum glutamic-pyruvic transaminase (SGPT) as well as total bilirubin were measured at baseline and day 14.
The liver function parameters were not remarkably changed at day 14 when compared to baseline and all liver function parameters were within the normal range (Table 9 and Fig. 8).
|
Table 9. Comparison of Mean Change in Liver Function Parameters from Baseline to Day 14
|
|
Parameters
|
Visit (V)
|
Mean ± SD
(n = 30)
|
Change from V1 (mean ± SD)
|
95% CI of Diff.
|
P value
|
|
SGOT (IU/L)
|
V1
V3
|
25.24 ± 9.49
25.34 ± 7.47
|
-0.10 ± 5.45
|
-2.134-1.935
|
0.92
|
|
SGPT (IU/L)
|
V1
V3
|
33.19 ± 12.41
31.99 ± 9.83
|
1.21 ± 8.44
|
-1.943-4.360
|
0.44
|
|
Total bilirubin (mg/dL)
|
V1
V3
|
0.65 ± 0.31
0.61 ± 0.26
|
0.04 ± 0.41
|
-0.112-0.194
|
0.59
|
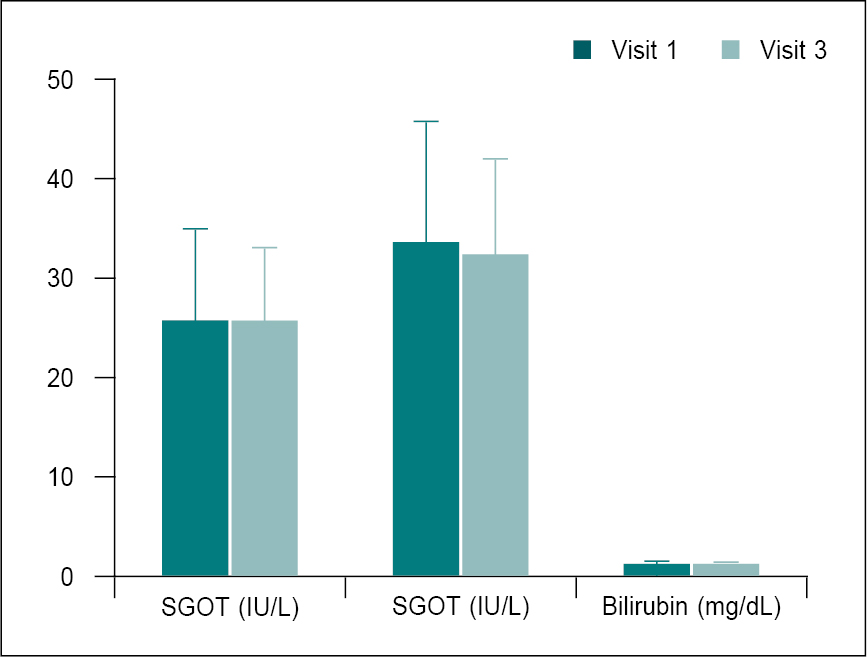
Figure 8. Comparison of mean change in liver function parameters from baseline (V1) to day14 (V3).
Liver function parameters at V1 were compared with V3 using paired t-test. Comparison: V1 vs. V3.
Adverse Events
No adverse effects or serious adverse effects were observed during the study period. However, one participant at visit 3 had diarrhea and this effect was found to be unrelated to Stomatab treatment.
DISCUSSION
- grandiflorum has antimicrobial, anti-inflammatory, antiseptic, wound healing properties among other beneficial effects.5 The wound healing activity of the ethanolic extract of flowers of J. grandiflorum was investigated in an experimental study. Rats treated with the extract in doses of 250 mg/kg body weight orally for 10 days showed significant decrease in the wound area compared to controls; 65% versus 54%, respectively. Well organized bands of collagen, greater number of fibroblasts and fewer inflammatory cells were seen on histopathological examination of the tissue on the 10th day in comparison to controls, which showed the presence of inflammatory cells, very little collagen fibers and fibroblasts suggesting the wound healing activity.6 The use of Jati or J. grandiflorum mouthwash was evaluated in patients with recurrent aphthous stomatitis. Patients were instructed to gargle with 10 mL of Jati mouthwash twice in a day for 1 week. By the 5th day of the treatment, associated symptoms of redness, swelling, burning sensation and difficulty in swallowing food disappeared completely. There was a marked decrease in pain. Healing of the ulcers occurred without scarring. This study demonstrated the accelerated healing of the aphthous ulcers within 5 days of initiation of treatment.7
- elengi has significant anti-inflammatory, analgesic and antipyretic properties, which were demonstrated in a study by Purnima et al using carrageenan-induced paw edema (acute inflammation) and cotton pellet-induced granuloma (sub-inflammation) models. The alcohol extract of M. elengi in a dose of 200 mg/kg caused marked inhibition of carrageenan-induced paw edema at 3rd (30.9%) and 4th hours (26%) compared to controls. In the cotton pellet-induced granuloma model, the extract was found to inhibited the increase in dry weight of cotton pellet granuloma by 29% versus saline control. The onset of action of antipyretic activity was 1 hour, which persisted for 5 hours.8 M. elengi has astringent and hemostatic properties due to the presence of tannins.9 Additionally, M. elengi has antimicrobial, antifungal, antioxidant and wound healing properties, which may be beneficial in aphthous ulcers.10
- religiosa has been shown to have anti-inflammatory, analgesic, antimicrobial, antiviral, antioxidant, immunomodulatory, antiulcer, antianxiety properties, which are useful in patients with stomatitis. Alcoholic extract of F. religiosa has wound healing property, which is aided by the antibacterial activity and the presence of tannins in leaf and stem extracts.11
The efficacy of Ashvattha or F. religiosa was examined in 30 patients with aphthous ulcers. The participants were grouped into two: Group A received Ashvattha twak choorna (powder) and honey; Group B was given Ashvattha twak choorna and water. Within 4 days, there was complete (100%) relief in toda (pricking pain) in Group A versus 93% in Group B. Alleviation of daha (burning sensation) was significant and occurred equally in both groups. Discoloration improved in 74% of patients in Group A versus 40% in Group B. Although results were significant in both groups, healing of the ulcers occurred more rapidly in Group A patients.12
Red ochre, known as Geru in Ayurveda, is a mixture of iron oxide (Fe2O3) and clay. It is an astringent and also has coagulating, cooling, antibilious and wound healing properties among others. It reduces the burning sensation (Daha).13,14 Red ochre has been shown to be effective in controlling bleeding in adolescents with menorrhagia via its astringent and styptic properties.15
CONCLUSION
The results of the study demonstrated that “Stomatab” capsule is highly effective for the treatment of mouth ulcer (stomatitis), as evidenced by the decrease in ulcer size, number of ulcers and related symptom scores. The constituent herbs of this polyherbal product act in a synergistic manner to relieve the symptoms of stomatitis. Furthermore, during the 14-day treatment period, no significant changes in vital signs, hematological profile, lipid profile, renal and liver functions were observed. No treatment-related side effects were reported by any of the study participants.
Conflict of Interest
The authors have no conflict of interest.
Sponsor
Bangalore Pharmaceutical & Research Laboratory (P) Ltd
No. 163, Reservoir St, Basavanagudi, Bengaluru, Karnataka
REFERENCES
- Porter SR, Scully C, Pedersen A. Recurrent aphthous stomatitis. Crit Rev Oral Biol Med. 1998;9(3):306-21.
- Hamdy AA, Ibrahem MA. Management of aphthous ulceration with topical quercetin: a randomized clinical trial. J Contemp Dent Pract. 2010;11(4):E009-16.
- Sakly A, De Wever B, Jutla B, Satia M, Bogaert JP. The safety and efficacy of AphtoFix® mouth ulcer cream in the management of recurrent aphthous stomatitis. BMC Oral Health. 2016;16:17.
- Gauthaman J, Ganesan A. Therapeutic evaluation of 5% topical amlexanox paste and 2% curcumin oral gel in the management of recurrent aphthous stomatitis - a randomized clinical trial. J Indian Acad Oral Med Radiol. 2022;34(1):17-21.
- Ali ST, Ayub A, Ali SN, Begum S, Siddiqui BS, Mahmood N, et al. Antibacterial activity of methanolic extracts from some selected medicinal plants. Fuuast J Biol. 2017;7(1):123-5.
- Nayak BS, Mohan K. Influence of ethanolic extract of Jasminum grandflorum flower on wound healing activity in rats. Indian J Physiol Pharmacol. 2007;51(2):189-94.
- Balakrishnan G, Vineeth PK, Mohanan AM, Ramesh NV. Effect of Jati (Jasminum grandiflorum) mouthwash in RAS: a case report. Int Res J Pharm. 2018;9(3):81-4.
- Purnima A, Koti BC, Thippeswamy AH, Jaji MS, Swamy AH, Kurhe YV, et al. Antiinflammatory, analgesic and antipyretic activities of Mimusops elengi Indian J Pharm Sci. 2010;72(4):480-5.
- Salve AV, Malik R, Ansari S, Uike S. Mimusops elengi (Linn.): an effective aid in dental care. J Global Oral Health. 2022;5:54-7.
- Rani S, Rahman K. Molsari (Mimusops elengi): a boon drug of traditional medicine. Int J Pharm Sci Res. 2017;8(1):17-28.
- Kapile C, Kulkarni A, Pardeshi P, Sayed A, Nehe A. Ficus religiosa: a beneficial medicinal plant. J Drug Deliv Ther. 2022;12(2-s):210-8.
- Nair VV, Rajashekhara N, Kavitha BM. Clinical evaluation of Ashvattha (Ficus religiosa) in Mukhapaka with special reference to aphthous ulcer. J Ayu Herb Med. 2015;1(3):77-80.
- Chavan SB, Gupta VS, Deshmukh VV, Sardeshmukh SP. Pharmaceutical standardization and physicochemical characterization of traditional ayurvedic mineral drug Red ochre roasted in cow’s ghee (Shuddha Gairik). Indian J Tradit Knowl. 2022;21(2):303-16.
- Lata S, Gupta L, Vardhan S, Kapil P, Sharma S. Concept of Shodhana of Gairik in Godugdha. Int J Ayu Pharm Chem. 2018;8(3):39-43.
- Kotagasti T. Efficacy of Geru (Red ochre) in controlling the bleeding in patients of adolescent menorrhagia. TANG [HUMANITAS MEDICINE]. 2015;5(2):e12-e15.