Abstract
Dengue fever is an arboviral infection, which is highly prevalent in tropical and subtropical climates. It is frequently associated with neurological complications but its association with ischemic stroke is ill defined. We present a case of an apparently healthy young male admitted with dengue fever complicated by ischemic infarct in corpus callosum. Our patient was managed conservatively, improved clinically and discharged in satisfactory condition.
Keywords: Dengue fever, neurological complications, ischemic stroke, infarct, corpus callosum
Dengue fever (DF) occurs frequently in tropical and subtropical countries worldwide, mostly in semi-urban and urban regions. It causes a wide-spectrum of disease ranging from subclinical illness to fatal dengue hemorrhagic fever and dengue shock syndrome. Neurological complications of dengue are attributed to: (1) viral neurotropism such as encephalitis, meningitis, etc.; (2) systemic complications such as stroke, encephalopathy; (3) post-viral immune-mediated acute disseminated encephalomyelitis, neuromyelitis optica, Guillain-Barré syndrome, etc.1
We present a case of an apparently healthy young male admitted with severe dengue fever complicated by ischemic infarct involving splenium of corpus callosum.
Case Report
A 22-year-old male presented to emergency with complaints of high-grade fever for 4 days associated with joint pains, nausea and generalized weakness.
On examination, patient had features of dehydration, dry lips and oral mucosa. He did not have any bleeding manifestations. His enzyme-linked immunosorbent assay (ELISA) for dengue virus antibody titers were 35.02 units (positive >11 units) and hemoglobin was 13.6 g%, total leukocyte count (TLC) 5800/mm3, platelets of 40,000/mm3. His serum glutamic-oxaloacetic transaminase/serum glutamic-pyruvic transaminase (SGOT/SGPT) levels were 2x the upper normal laboratory reference value.
Total bilirubin and international normalized ratio (INR) were normal. His acute phase reactants were elevated with C-reactive protein (CRP) being 17.2 mg/L and ferritin >16,500 ng/mL. His chest X-ray showed haziness in bilateral costophrenic angle consistent with pleural effusion. He was started on intravenous fluids and symptomatic treatment. The patient developed an episode of confusion with no focal neurological deficit on the next day.
In view of that, patient underwent magnetic resonance imaging (MRI) brain, which showed focal areas of acute diffusion restriction signal intensity in the splenium in the midline portion, appearing hyperintense on diffusion-weighted image (DWI)/T2/FLAIR (fluid-attenuated inversion recovery) images with a drop in signal intensity on apparent diffusion coefficient (ADC) mapping, findings consistent with acute ischemic infarct (Fig. 1). His 2D echocardiogram was normal with no left ventricular dysfunction or evidence of thrombi. His carotid duplex ultrasound was also normal. Conservative management was continued and his acute confusion state recovered subsequently.
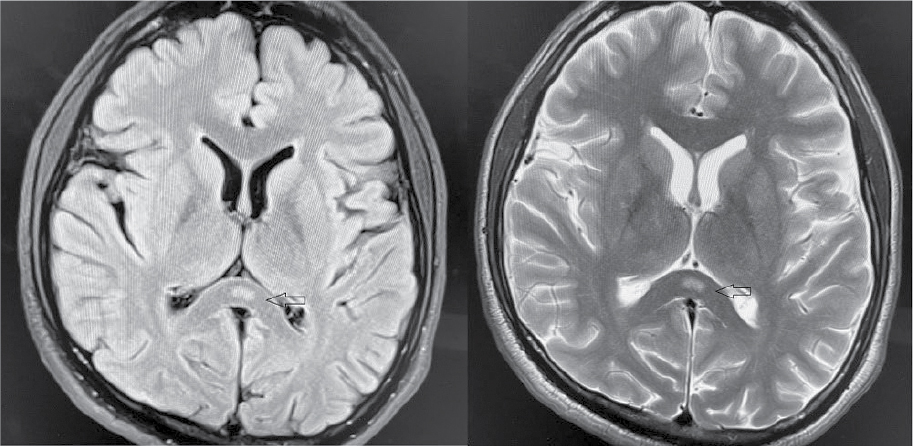
Figure 1. Focal areas of acute diffusion restriction signal intensity in the splenium in the midline portion (marked by arrow), appearing hyperintense on DWI image, findings consistent with acute ischemic infarct in splenium of corpus callosum.
On Day 7, his platelets increased to above 1 lakh/mm3; liver enzymes, CRP and ferritin normalized. He was discharged in a satisfactory condition.
DISCUSSION
Dengue viruses are transmitted in humans by female Aedes mosquitoes with Aedes aegypti being the most important vector in the tropical and subtropical regions. The virus has four antigenically similar serotypes (DENV 1-4). Dengue fever is endemic in 128 countries; most of them are developing nations, posing an annual threat to approximately 3.97 billion people.2
The exact incidence of various neurological complications is undetermined.1 Encephalopathy and encephalitis are the most frequently reported neurological complications of dengue, with incidence found to vary between 0.5%3 and 6.2%.4 Verma et al evaluated 26 patients with neurological manifestation in dengue fever. No patient in their study had ischemic stroke.5 Contrary to that Li et al concluded that, there is time-dependent increase in risk of stroke in dengue patients compared to control6 and also reported more of ischemic stroke than hemorrhagic stroke suggesting possibility of underreporting of cases.
Conclusion
Our patient is a 22-year-old male with no comorbidities or risk factors for ischemic stroke. As his echocardiogram did not reveal any thrombus or ventricular dysfunction and carotid artery duplex imaging was normal, we presume that in this patient dengue fever is the probable cause for the infarction.
Ischemic stroke is an unusual manifestation in patients with dengue fever. One would expect thrombocytopenia-related acute hemorrhagic infarct to be present in such patients rather than ischemic infarct.
REFERENCES
- Murthy J. Neurological complications of dengue infection. Neurol India. 2010;58:581-4.
- Khetarpal N, Khanna I. Dengue fever: causes, complications, and vaccine strategies. J Immunol Res. 2016;2016:6803098.
- Cam BV, Fonsmark L, Hue NB, Phuong NT, Poulsen A, Heegaard ED. Prospective case-control study of encephalopathy in children with dengue hemorrhagic fever. Am J Trop Med Hyg. 2001;65(6):848-51.
- Hendarto SK, Hadinegoro SR. Dengue encephalopathy. Acta Paediatr Jpn. 1992;34(3):350-7.
- Verma R, Sharma P, Garg RK, Atam V, Singh MK, Mehrotra HS. Neurological complications of dengue fever: experience from a tertiary center of north India. Ann Indian Acad Neurol. 2011;14(4):272-8.
- Li HM, Huang YK, Su YC, Kao CH. Risk of stroke in patients with dengue fever: a population-based cohort study. CMAJ. 2018;190(10):E285-90.