Published in IJCP
June 2023
Clinical Study
Vascular Calcification in Chronic Kidney Disease Patients on Hemodialysis: Prevalence and Correlation with Vascular Disease Events
June 10, 2023 | Fayaz Ahmad War, Manju Aggarwal, Sourabh Sharma
Nephrology
Abstract
Introduction: With declining kidney function, the prevalence of vascular calcifications increases and calcification occurs years earlier and is more severe in chronic kidney disease (CKD) patients than in general population. We did this study to find the prevalence of vascular calcification in patients on maintenance hemodialysis using simple and inexpensive radiological method and to find out the correlation of vascular calcification score with vascular disease events, cardiovascular and all-cause mortality over a follow-up period of 1 year. Materials and methods: This prospective, observational, comparative, follow-up, single-center study of maintenance hemodialysis patients was performed at a tertiary care center in Haryana. Seventy-one patients on maintenance hemodialysis for more than 3 months were included in the study. Patients who were 18 years of age or below, CKD stage 5 patients not on dialysis and those who had previous history of parathyroidectomy were excluded. Adragao score for vascular calcification was calculated by evaluating bilateral iliac, femoral and radial arteries in plain radiographic films of pelvis and hands. Statistical analyses were performed with the SPSS System 10.0. Results: Seventy-one patients were enrolled in this study out of which, 45 were male and 26 were female. Mean age of patients was 61.92 ± 10.77 years. Majority of patients were elderly (age group ≥60 years). Out of 71 patients, 66 (92.9%) were hypertensive and 26 (36.6%) patients were diabetic. Twenty-two (30.9%) patients had cardiovascular disease (CVD) at baseline. Coronary artery disease (CAD) was present in 20 (28.1%) patients, cerebrovascular disease was present in 2 (2.8%) patients and peripheral artery disease (PAD) was present in only 1 patient at baseline. Average dialysis duration received by patients was 21.35 ± 21.17 months. Out of 71 patients, 16 (22.5%) received calcium-containing phosphate binder, 51 (71.8%) received noncalcium-containing phosphate binder and 4 patients received no phosphate binder. Fifty-five (77.4%) patients received therapeutic or prophylactic vitamin D3 therapy during the study period. Vascular calcification detected with plain X-ray of pelvis and both wrists was found in 56.3% of patients on maintenance hemodialysis. The prevalence and severity of vascular calcification was higher with increasing age. Diabetes was found to be significantly associated with the presence of vascular calcification (p < 0.0005). CAD at the time of enrollment was significantly associated with vascular calcification (p = 0.009). Serum levels of calcium, phosphate, vitamin D3, intact parathyroid hormone (PTH), calcium-phosphate product or use of phosphate binders or the types or vitamin D therapy did not correlate clinically with presence of vascular calcification. Hemodialysis duration did not correlate with the presence of vascular calcification (p = 0.113). Presence of vascular calcifications in hemodialysis patients predicted future vascular disease events over 1 year follow-up (p = 0.013) but did not correlate with cardiovascular and all-cause mortality. Conclusion: There is a high prevalence of vascular calcification in maintenance hemodialysis patients in our center. The risk factors of vascular calcification were higher age, diabetes and CAD. These patients should be followed-up regularly for vascular events. We also want to reiterate with this study that plain X-ray is sufficient to rule out vascular calcification in CKD patients and should be employed regularly in dialysis clinics.
Keywords: Vascular calcification, chronic kidney disease, hemodialysis, vascular diseases
Vascular calcification is a process characterized by thickening and loss of elasticity of muscular artery walls. There are two main types of vascular calcifications in chronic kidney disease (CKD) patients on hemodialysis: (i) common atherosclerosis, with intimal patchy calcifications of atherosclerotic plaques and (ii) medial sclerosis with medial linear calcifications that seem to be related to mineral metabolism disturbances.1 Arterial medial calcification is an active process in response to pathological conditions, including aging,2 inflammation, diabetes, CKD and phenotypic switch of resident cells.3 With declining kidney function, the prevalence of vascular calcifications increases and calcification occurs years earlier and is more severe in CKD patients than in the general population. The phenotype of vessels of younger dialysis patients is comparable with that of octogenarians without CKD.4 The prevalence of vascular calcifications among patients with CKD, especially those on hemodialysis, is extremely high (>80%);5 its prevalence increases with progressive fall in glomerular filtration rate (25% in stage 3 and 35% in stage 4)6 and is present in over 50% of patients at the time of initiation of renal replacement therapy (RRT).7 Some concern has been raised that the high prevalence and severity of vascular calcification among CKD patients may be related to the administration of calcium-containing phosphate binders used to treat hyperphosphatemia. However, vascular calcification was a frequent feature of patients with CKD prior to the availability of calcium-containing phosphate binders.8
This suggests that calcium-containing phosphate binders alone do not explain the high prevalence of vascular calcifications among CKD patients. It is possible that the increasingly high prevalence may be the result of a greater number of elderly and diabetic patients, and better technologies for assessment and quantification of vascular calcification. Several risk factors may induce arterial calcification leading to accelerated vascular aging. They are divided into “classic” risk factors such as age, gender, CKD and dialysis vintage, inflammatory status, disorders of calcium and phosphate, diabetes and “non-classic” factors such as abnormal levels of bone-related proteins: fetuin-A, matrix-carboxyglutamic acid protein (Matrix-Gla protein, MGP), pyrophosphate, osteoprotegerin and bone morphogenetic protein-2.9
These factors also influence each other, for example, the reduction of renal function promotes the development of inflammation (increase of C-reactive protein and reduction of fetuin-A) that contribute to endothelial dysfunction and vascular calcification. Increasing age and time on dialysis are major risk factors for vascular calcification. This was demonstrated in a comprehensive systematic review of 30 studies over a period of 20 years that showed that age and length of time on dialysis therapy were the main factors associated with vascular calcification among patients with CKD.10 Among patients without CKD; many studies have shown that diabetes is a risk factor for vascular calcification. Among CKD patients, diabetes also increases the risk of vascular calcification. Poorly controlled hyperphosphatemia often increases the requirement for calcium-containing phosphate binders, which then increases the risk of recurrent concomitant hypercalcemia. Most experts believe that a raised plasma phosphate with intermittent or persistent hypercalcemia drives the initiation and progression of vascular calcification.11 There appears to be relatively less progression of vascular calcification with sevelamer versus calcium-containing phosphate binders among dialysis patients. Clinically employed doses of vitamin D frequently result in hypercalcemia and an elevated calcium-phosphate (Ca x P) product, which can accelerate extraosseous calcification.12
Important mechanisms of vascular calcification in CKD patients are the failure of inhibitory systems for vascular calcification and differentiation of vascular smooth muscle cells (VSMCs) to osteoblast-like cells. Inhibitory factors for vascular calcification include MGP, pyrophosphate (produced in VSMCs) and circulating inhibitor fetuin-A. On the other hand, activation of transcription factors “Runx2” and mineralization regulating protein “alkaline phosphatase (ALP)” are important key factors for osteochondrocytic differentiation of VSMCs. Uremic milieu concomitantly inactivates the production of inhibitors and promotes phenotypic changes and/or apoptosis of VSMCs resulting in medial calcification.13 Several reports have shown the strong relationship between vascular calcification and clinical outcomes including cardiovascular events, and cardiovascular and all-cause mortality. The number of calcified sites was a strong predictor of cardiovascular and all-cause mortality.14 Dialysis patients with higher vascular calcification scores have significantly higher rate of cardiovascular events, cardiovascular and all-cause mortality compared with those with mild or no calcification score.15 A number of noninvasive methods have been developed for the detection and quantification of vascular calcification. Electron-beam computed tomography (EBCT) scan detects and quantifies vascular calcification, and is a more sensitive method for detection of vascular calcifications. However, it is a very expensive method and does not differentiate between intimal and medial calcium deposition. The simplest technique is plain radiography, which demonstrates pipe-stem calcification of the tunica media and more irregular, patchy calcifications of the internal elastic lamina. Plain films may differentiate between intimal and medial calcification to some degree.16
Plain films are, however, less sensitive compared to EBCT. The use of plain radiographic films for vascular calcification assessment has been suggested in the recent KDOQI clinical practice guidelines.17 The main aim of this study was to find the prevalence of vascular calcification in patients who are on maintenance hemodialysis in our center using a simple and inexpensive radiological method for diagnosis of vascular calcifications, and to find out the correlation of vascular calcification score with vascular disease events (coronary artery disease [CAD], cerebrovascular disease and peripheral artery disease [PAD]), cardiovascular and all-cause mortality over a follow-up period of 1 year. The timely diagnosis of vascular calcifications and the identification of possible contributing factors raise the hope for a possible primary, and therapeutic intervention that might reduce cardiovascular and other vascular diseases risk in hemodialysis patients.
MATERIALS AND METHODS
Place of Study
Department of Nephrology, Artemis Hospitals, Gurugram, Haryana, India.
Study Design
This was a prospective, observational, comparative, follow-up, single-center study of maintenance hemodialysis patients.
Patient Population
Seventy-one patients who were on maintenance hemodialysis for more than 3 months were included in the study. Patients who were 18 years of age or below, end-stage renal disease (ESRD) patient not on dialysis and those who had previous history of parathyroidectomy were excluded from the study. Among the enrolled patients, those who had no vascular calcifications, were taken as controls.
Collection of Data
A proforma providing all historical, clinical and treatment details during the course of study was used to record patient data. The following data of all patients was collected at the time of enrollment in the study: demographic profile, basic renal disease, hemodialysis duration, comorbidities like diabetes, hypertension, CAD at baseline, phosphate binder used, vitamin D therapy and calcium intake. Serum calcium, serum phosphorus, ALP, serum albumin, serum 25-hydroxyvitamin D [25(OH)D] levels and intact parathyroid hormone (PTH) were measured in all the patients. Dialysate calcium concentration of 1.75 mmol/L was used in our Dialysis center for all patients. All patients were subjected to plain X-rays (anteroposterior view) of pelvis and both wrists at the time of inclusion in the study. The X-rays were reported by an experienced radiologist who was blinded to the clinical profile of patients. A simple vascular calcification score developed by Adragao et al18 was used to evaluate vascular calcifications.
Adragao Score
This vascular calcification score was evaluated from bilateral iliac, femoral and radial arteries in plain radiographic films of pelvis and hands. The pelvis radiographic films were divided into four sections by two imaginary lines: a horizontal line over the upper limit of both femoral heads and a median vertical line over the vertebral column. The films of the hands were divided, for each hand, by a horizontal line over the upper limit of the metacarpal bones. The presence of linear calcifications in each section was counted as 1 and its absence as 0. The final score was the sum of all the sections, ranging from 0 to 8.18 Vascular calcifications were deliberately evaluated only in muscular arteries: iliac, femoral, radial and digital. Pelvic films evaluated iliac and femoral arteries (Fig. 1); wrist films evaluated radial and digital arteries (Fig. 2). Only linear calcifications, with or without patchy calcifications, were considered for the final calcification score, because they outline the vessel wall and have undoubtedly vascular localization. Patchy isolated calcifications that may be associated with intimal calcifications were not considered in this score.
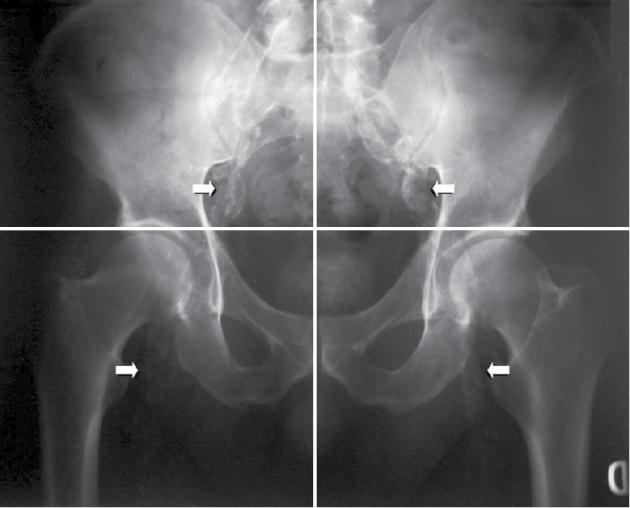
Figure 1. Vascular calcification score - Pelvic films to evaluate iliac and femoral arteries.
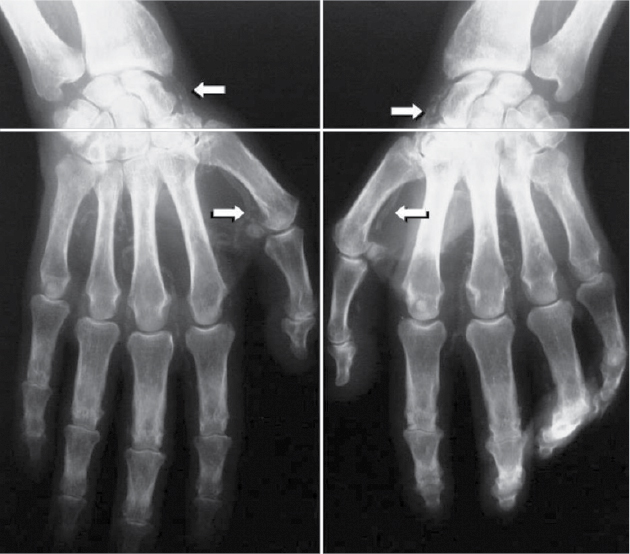
Figure 2. Vascular calcification score - Wrist films to evaluate radial and digital arteries.
Serum calcium was measured by indirect ion selective electrode method and serum phosphate by phosphomolybdate method, on UniCel DxC 800 Synchron Clinical System. ALP was measured by P-nitrophenyl phosphate AMP-Buffer method and albumin by bromocresol purple method, both were measured on UniCel DxC 800 Synchron Clinical System. Vitamin D (25-hydroxy) was measured by enzyme-linked fluorescent assay on MiniVIDAS which is a multiparametric immunoanalyzer. Intact PTH levels were measured using chemiluminescence immunoassay on UniCel DxC 860i Synchron Access Clinical System. Patients were followed over a period of 12 months from March 2016 to February 2017.
All vascular disease events (CAD, CVD and PAD), were recorded in detail over 1 year. CAD was diagnosed if the patient developed typical angina pectoris, had positive stress test, had acute coronary syndrome (ACS), or underwent percutaneous transluminal coronary angioplasty (PTCA) or coronary artery bypass surgery (CABG), or if the patients had regional wall motion abnormality (RWMA) on 2D Echo. The diagnosis of cerebrovascular disease was based on occurrence of stroke or transient ischemic attack (TIA) or detection of old infarct on CT/MRI (magnetic resonance imaging) brain. PAD was diagnosed if there was history of claudication, ischemic ulcers, lower limb amputations or diagnosis by Doppler or angiography.
ETHICAL CONSIDERATION
Before the commencement of study, informed and written consent was obtained from all the patients selected for the study after explaining the risks and benefits associated with the study. The aim and the value of work was explained to them. Participation of patients was voluntary and their data was kept confidential.
STATISTICAL ASPECTS
Variables were expressed as frequencies, percentages for discrete factors and mean values for normally distributed continuous factors. Statistical comparisons of baseline characteristics and end points were performed using the two-tailed Chi-square test. The independent variables associated with vascular calcifications, vascular disease at baseline and vascular disease at the end of follow-up were identified by binary logistic regression models. Covariates for vascular calcification analysis were age, sex, diabetes, hemodialysis duration, calcium, phosphate, Ca x P product, vitamin D3 and intact PTH. Statistical analyses were performed with the SPSS System 10.0. For all comparisons, a p-value of <0.05 was considered statistically significant.
RESULTS
Seventy-one patients were enrolled in this study out of which, 45 were male and 26 were female. The demographic characteristics of the patients has been depicted in Table 1. Mean age of patients was 61.92 ± 10.77 years. Majority of patients were elderly (age group of 60 or above). Out of 71 patients, 66 (92.9%) were hypertensive and 26 (36.6%) were diabetic. Twenty-two (30.9%) patients had CVD at baseline. CAD was present in 20 (28.1%) patients, cerebrovascular disease was present in 2 (2.8%) patients and PAD was present in only 1 patient at baseline. Average dialysis duration received by patients was 21.35 ± 21.17 months. Out of 71 patients, 16 (22.5%) received calcium-containing phosphate binder, 51 (71.8%) received noncalcium-containing phosphate binder and 4 patients received no phosphate binder. Fifty-five (77.4%) patients received therapeutic or prophylactic vitamin D3 therapy during the study period.
|
Table 1. Demographic, Clinical and Laboratory Characteristics of Patients Studied
|
|
Patient characteristic
|
Mean ± SD or No. (%) of patients
|
|
Age
|
61.92 ± 10.77
|
|
Male
|
45 (63.38)
|
|
Female
|
26 (36.61)
|
|
Basic disease
Diabetic nephropathy
Nondiabetic
|
26 (36.61)
45 (63.3)
|
|
Comorbidities
Hypertension
Diabetes
CVD
Others
|
66 (92.95)
26 (36.61)
22 (30.98)
40 (56.33)
|
|
Serum calcium
|
8.33 ± 0.79
|
|
Serum albumin
|
3.36 ± 0.47
|
|
Corrected calcium
|
8.81 ± 0.85
|
|
Serum phosphorus
|
5.96 ± 2.03
|
|
Ca x P product
|
51.87 ± 16.38
|
|
ALP
|
84.78 ± 39.65
|
|
Vitamin D3
|
29.02 ± 12.25
|
|
Intact PTH
|
266.6 ± 270.2
|
Prevalence of Vascular Calcification
- Age: Prevalence of vascular calcification (calcification score of ≥1) was 56.3%, which increased with increasing age of patients, for example, prevalence of vascular calcification was 60.4% in patients aged 60 years or above, whereas prevalence of vascular calcification was 50% in patients below 60 years of age. Severity of vascular calcification also increased with age, for example, 39.5% of patients above 60 years of age had vascular calcification score of 4 or above, whereas only 28.5% of patients between 40 to 60 years of age had vascular calcification score of 4 or above (Fig. 3).
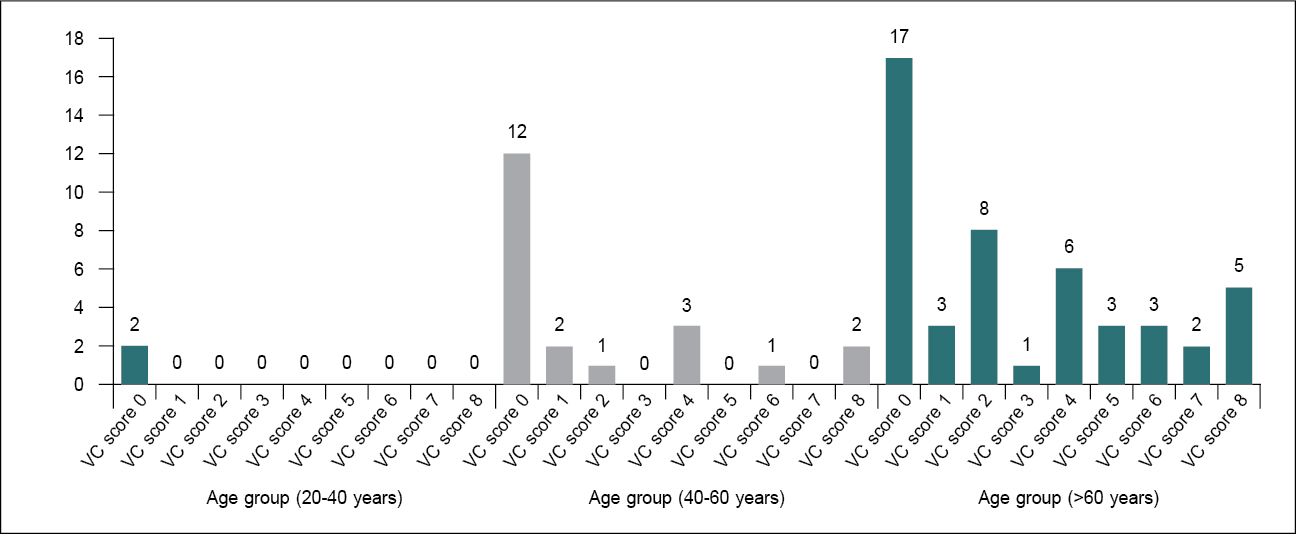
Figure 3. Vascular calcification score in different age groups.
VC = Vascular calcification.
- Sex: Prevalence of vascular calcification was similar in male and female patients. Out of 45 male patients, 25 (55.5%) had vascular calcifications and out of 26 female patients, 15 (57.6%) had vascular calcification.
- Diabetes: Prevalence of vascular calcification was significantly higher in hemodialysis patients who were diabetic (92.3%) compared to nondiabetic (35.5%) patients (p < 0.0005).
- Hypertension: Out of 66 hypertensive patients, 37 (56%) had vascular calcifications ranging from total vascular calcifications score of 1 to 8, whereas out of 5 normotensive patients, 3 (60%) had vascular calcification (p = 0.864).
- CVD at baseline: Out of 71 patients, there were 22 patients with CVD at baseline. Vascular calcification was present in 63.5% of patients with CVD at baseline, whereas it was present in 53% of patients without CVD at baseline (p = 0.406).
- CAD at baseline: Vascular calcification was more common in patients who had CAD at baseline compared to those who had no CAD at baseline (60% 54.9%; p = 0.009). Moreover, among patients who had vascular calcifications, 30% had CAD at baseline compared to 25.8% in those with no vascular calcification (Table 2).
|
Table 2. Vascular Calcification Score in Patients With and Without CAD at Baseline
|
|
CAD (at baseline)
|
Vascular calcification score
|
P value
|
|
0
|
1-4
|
4-8
|
|
Yes (n = 20)
|
8 (40%)
|
3 (15%)
|
9 (45%)
|
0.009
|
|
No (n = 51)
|
23 (45%)
|
21 (41.1%)
|
7 (13.7%)
|
- Cerebrovascular disease at baseline: Only 2 patients had cerebrovascular disease at baseline and both the patients had vascular calcifications (p = 0.589).
- Peripheral vascular disease at baseline: Out of 71 patients, only 1 patient had peripheral vascular disease at baseline and vascular calcification was present in that patient (p = 0.896).
- Hemodialysis duration: Vascular calcification was present in 63.6% of patients on hemodialysis for 1 year or above at enrollment, whereas it was present in only 44.4% of patients who were on hemodialysis for less than 1 year. However, this difference was not statistically significant (p = 0.113).
- Serum calcium level: Mean corrected serum calcium level was 8.33 ± 0.79. All the values were within the range of 7.2 mg/dL to 12.1 mg/dL. Majority of patients (n = 67) had normal or slight lower serum calcium levels, only 4 patients had hypercalcemia. Serum calcium level was not associated with vascular calcification (p = 0.193).
- Serum phosphate levels: Mean serum phosphorus level was 5.96 ± 2.03 mg/dL. Only 21 patients had achieved serum phosphorus levels within normal range meeting the recent KDIGO guidelines, out of which 14 had vascular calcifications, whereas 50 patients had serum phosphorus above the normal range, out of whom 26 had vascular calcifications. Therefore, hyperphosphatemia was not associated with presence of vascular calcification (p = 0.255).
- Calcium-phosphate product: Mean Ca x P product was 51.87 ± 16.38. In patients with Ca x P product >50, 54% had vascular calcifications whereas in patients with Ca x P product <50, 58.8% had vascular calcifications. Therefore, high Ca x P product does not appear to contribute to vascular calcification (p value 0.685).
- Serum vitamin D3 levels: Mean serum vitamin D3 level was 29.02 ± 12.25. Majority of patients (n = 43) had vitamin D3 levels ≤30, and 28 patients had vitamin D3 levels >30. There was no significant difference in prevalence of vascular calcification between the two groups base on vitamin D3 levels (p = 0.548).
- Serum intact PTH: Mean serum intact PTH levels was 266.6 ± 270.228 pg/mL. Thirteen patients had intact PTH levels below 150 pg/mL and 21 patients had intact PTH levels above 300 pg/mL, whereas only 22 (30.9%) met KDOQI guidelines for PTH (150-300 pg/mL). Paradoxically vascular calcification was most commonly (68.1%) seen in this group (p = 0.304).
- Phosphate binder used: Out of 71 patients, 16 patients were receiving calcium-containing phosphate binder and 51 were receiving noncalcium-containing phosphate binders. Around 62.5% patients on calcium-containing phosphate binders had vascular calcification, whereas 50.9% of patients on noncalcium-containing phosphate binders had vascular calcification. Therefore, vascular calcification was more common in patients taking calcium-containing phosphate binders, however, this difference was not statistically significant (p = 0.42).
- Vitamin D therapy: Out of 71 patients included in the study, 55 received prophylactic or therapeutic doses of vitamin D3 and among these patients, 34 (61.8%) had vascular calcifications whereas only 6 (37.4%) out of 16 patients not receiving vitamin D3, had vascular calcifications. Therefore, vascular calcification was more common in patients on vitamin D therapy; however, this difference was not statistically significant (p = 0.084).
Vascular Disease Events During 1-year Follow-up
Total number of vascular disease (CAD, cerebrovascular disease, PAD) events that occurred over a follow-up period of 12 months were 9 and all events occurred in patients who had vascular calcification score ≥1 at the time of enrollment in the study (p = 0.013). Out of the total number of patients included in the study, 30.9% had CVD at baseline, which increased to 38% at the end of the study. However, in patients with vascular calcification, 35% had CVD at the time of enrollment, which increased to 47.5% at the end of the study.
Cardiovascular Deaths During 1-year Follow-up
During the 1 year follow-up, out of 40 patients who had vascular calcifications, 1 patient died of a cardiovascular cause (p = 0.896). No deaths occurred in the patient group who had no vascular calcifications.
All-cause Deaths During 1-year Follow-up
Out of 71 patients enrolled in the study, there were 6 deaths over a follow-up period of 1 year. All the deaths occurred in patients with vascular calcification. No death was reported in the patient group with no vascular calcifications (p = 0.068).
New CAD Events Over 1-year Follow-up
There were 5 new CAD events over 1-year follow-up; all the events occurred in patients who had vascular calcifications at the time of inclusion in the study. No new coronary event occurred in patients without vascular calcifications (p = 0.115). No cerebrovascular event (stroke, TIA) occurred in either group. However, two new peripheral vascular disease events occurred in the vascular calcification group, whereas no new peripheral vascular disease event was noted in patients with no vascular calcification.
New vascular events were more common in patients with total vascular calcification score of ≥4 compared to those with vascular calcification score <4. However, the difference was not statistically significant (p value 0.32).
There were 6 all-cause deaths, 4 in patients with total vascular calcification score of ≥4 and 2 in patients with score of <4. There was only 1 death due to cardiovascular-cause and that occurred in the patient with total vascular calcification score of ≥4 (p = 0.215).
DISCUSSION
Vascular (medial) calcification is an active process that occurs due to failure of inhibitory mechanisms for calcification within VSMCs and differentiation of VSMCs into osteoblast-like cells. This type of vascular calcification is seen as railroad pattern on a plain radiograph.18
In this study, vascular calcifications were deliberately evaluated only in muscular arteries: iliac, femoral, radial and digital, because muscular arteries are more prone to linear calcification in contrast with elastic arteries that are more prone to intimal calcification. Vascular calcification causes arterial wall stiffness,19 which results in increased cardiac afterload leading to left ventricular hypertrophy. These functional and structural changes associated with vascular calcification have strong clinical impact on cardiovascular morbidity and mortality in dialysis patients. Also, if the prevalence of both vascular calcification and CVD is high in hemodialysis patients, the association between the two observations seems logical. Indeed, several observational studies confirmed this association, suggesting linear relationship between vascular calcification and cardiovascular morbidity and mortality.14,20-22
The prevalence of vascular calcifications among patients with CKD especially those on dialysis is very high. Kraus et al found a prevalence of abdominal aortic calcification of 77.8%, on lateral lumbar X-rays in ESRD patients on hemodialysis.20 Using plain radiograph of pelvis and wrists, Adragao et al found a prevalence of 74.7%.18 However, prevalence of vascular calcification in patients on hemodialysis is found to be >80%, using EBCT.5
In this study, prevalence of vascular calcification detected with plain X-ray of pelvis and both wrists, was 56.3% which is lower than observed in other studies as discussed. Higher mean age of patients and longer dialysis duration could be the reasons for higher prevalence of vascular calcification in these studies. Older age is considered one among the major risk factors for vascular calcification, which was demonstrated in a comprehensive review of 30 studies over a period of 20 years; it showed that age and dialysis duration were the main factors associated with vascular calcification among hemodialysis patients.10 Older age was associated with vascular calcification in other studies as well.23,24 In our study, prevalence of vascular calcification was 60.4% in patients aged 60 years or above, whereas it was 50% in patients below 60 years of age. Severity of vascular calcification also increased with age confirming the findings of above studies. In this study, prevalence of vascular calcification was found to be significantly higher in patients with diabetes. These findings are consistent with the study published in 2003 by London et al.16
The Dallas Heart Study in 2005 demonstrated that CKD is associated with increased coronary artery calcification score but this association may be substantially stronger among patients with diabetes.25 However, abdominal aortic calcification did not differ by diabetes status in another study, perhaps because fewer than 20% patients had diabetic nephropathy.20 In this study, vascular calcification did not correlate with blood pressure, which is consistent with another study in which no association was found between vascular calcification and hypertension;16 hypertension is considered a risk factor for atherosclerosis and not for vascular calcification. Vascular calcification was not significantly associated with overall CVD present at the time of enrollment in the study, which is consistent with the study by Adragao et al, in which clinical vascular disease diagnosed at baseline did not correlate with vascular calcification score.18 Vascular calcification was more common in patients who had CAD (prior myocardial infarction [MI], CABG or coronary angioplasty/stenting) present at baseline compared to those with no CAD at baseline. This was in line with other studies, in which the patients with prior evidence of ischemic heart disease and dysrhythmia had increased abdominal aortic calcification.20,24
In another study in hemodialysis recipients, coronary artery calcification was related to prevalent MI and angina and aortic calcification was related to prevalent PAD.26 The vascular calcifications may be present in patients when RRT is started.27 However, vascular calcification could be expected to increase with dialysis duration. In the study of Goldsmith and colleagues, in patients on hemodialysis for 10 to 25 years, radiographic vascular calcification prevalence increased from 39% at dialysis onset to 92% after an average dialysis duration of 16 years, with a mean onset 9.7 years after starting dialysis;12 calcification severity also increased with age. Another study also showed that the prevalence and progression of vascular calcification increases once patients are on dialysis.28 Similarly, in CORD study, dialysis duration independently predicted abdominal aortic calcification on multivariate analysis.24
In the current study, vascular calcification did not increase with dialysis vintage, perhaps due to shorter mean dialysis duration in our patients compared to above studies. This finding is also consistent with the results of another study in which the overall abdominal aortic calcification score did not increase with dialysis duration.20 Most experts believe that a raised plasma phosphate and calcium level leads to the initiation and progression of vascular calcification.11 However, vascular calcification was not correlated with serum calcium, serum phosphorus and intact PTH levels in our study. Similarly, Guérin et al did not find any association between a semiquantitative vascular calcification score evaluated by B-mode ultrasonography and calcium, phosphorus and intact PTH levels.17 Final vascular calcification score was also not correlated with serum calcium, phosphorus and intact PTH in the study done by Adragao et al.18 Majority of hemodialysis patients are vitamin D deficient and receive therapeutic or prophylactic doses of vitamin D3. In our study, serum level of 25(OH)D3 was not associated with the vascular calcification, as also reported by London et al.29
However, in another study of vascular calcification in hemodialysis patients, levels of vitamin D metabolites correlated with the extent and progression of vascular calcifications.12 Vascular calcification was not associated with vitamin D therapy in our study, probably, because majority of our patients received prophylactic doses of vitamin D3 rather than therapeutic doses that might increase the risk of hypercalcemia, Ca x P product which could increase the chances of vascular calcification. Noncalcium-containing phosphate binders have been associated with delayed progression of vascular calcification compared with calcium-containing phosphate binders. This was demonstrated by several studies.30-32
In this study, vascular calcification was more common in patients taking calcium-containing phosphate binders compared to those taking noncalcium-containing phosphate binder; however, this difference was not statistically significant. However, the CARE-2 trial did not find a difference in progression of coronary artery calcification with sevelamer and calcium acetate.33 Also, a meta-analysis that analyzed 14 researches could not find sevelamer hydrochloride more effective than calcium-based phosphate binders for delaying the progression of coronary artery calcification.34 Cardiovascular calcification predicts future cardiovascular morbidity and mortality in general population and dialysis patients. In the prospective general-public Framingham Heart Study with 22 years of follow-up, vascular calcification was associated with increased relative risk of CVD, coronary heart disease and cardiovascular mortality.35 Several studies have also demonstrated association between vascular calcification and cardiovascular morbidity and mortality, and all-cause mortality in hemodialysis patients.21,22,36-38 The number of calcified sites was a strong predictor of cardiovascular and all-cause mortality.14 Importantly, the associations found in these studies persisted after correcting for established risk factors. Moreover, longitudinal studies revealed that the progression rate of vascular calcification is also associated with the incidence of subsequent cardiovascular complications.39 In the present study, vascular disease events at the end of the follow-up was strongly associated with the presence of vascular calcification, which is consistent with other 54 studies.18,39
However, unlike the above study, total vascular calcification score was not an independent predictor of cardiovascular events, cardiovascular mortality and all-cause mortality in our study. In this study, presence of vascular calcification and total calcification score did not correlate with cardiovascular and all-cause mortality, which is not consistent with other studies,21,40,41 the likely reason could be the shorter follow-up period in our study. However, higher peripheral vascular calcification on X-rays was associated with increased mortality rate in 161 French hemodialysis patients followed over a period of 1 year;23 the mean age of patients was higher, with longer dialysis duration in this study. PAD is highly prevalent in hemodialysis patients, but is often under-diagnosed. The risk factors such as age and diabetes, hypercalcemia and hyperphosphatemia have been associated with higher risk of amputation suggesting a contributory role of vascular calcifications for PAD in this population.42,43 Furthermore, lower limb arterial calcification is closely associated with the presence and severity of PAD in hemodialysis patients.43 This was also confirmed by another study in which vascular calcification score was independently associated with PAD at the end of follow-up.18
However, this study did not show correlation between vascular calcification and peripheral vascular disease at the end of follow-up, likely because of shorter follow-up and smaller sample size.
CONCLUSIONS
There was a high prevalence of vascular calcification in maintenance hemodialysis patients in our center. There is a need to sensitize clinicians towards the high risk of vascular calcification in CKD population. The risk factors of vascular calcification are higher age, diabetes and CAD. These patients should be followed-up regularly for vascular events. We also want to reiterate with this study that plain X-ray of pelvis and wrists are sufficient to rule out vascular calcification in CKD patients and should be employed regularly in dialysis clinics.
REFERENCES
- Giachelli CM, Jono S, Shioi A, Nishizawa Y, Mori K, Morii H. Vascular calcification and inorganic phosphate. Am J Kidney Dis. 2001;38(4 Suppl 1):S34-7.
- London G, Covic A, Goldsmith D, Wiecek A, Suleymanlar G, Ortiz A, et al; European REnal and CArdiovascular Medicine working group of the European Renal Association–European Dialysis and Transplant Association (ERA–EDTA). Arterial aging and arterial disease: interplay between central hemodynamics, cardiac work, and organ flow-implications for CKD and cardiovascular disease. Kidney Int Suppl (2011). 2011;1(1):10-2.
- Cozzolino M, Brancaccio D, Gallieni M, Slatopolsky E. Pathogenesis of vascular calcification in chronic kidney disease. Kidney Int. 2005;68(2):429-36.
- Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998;32(5 Suppl 3):S112-9.
- Goodman WG, Goldin J, Kuizon BD, Yoon C, Gales B, Sider D, et al. Coronary-artery calcification in young adults with end-stage renal disease who are undergoing dialysis. N Engl J Med. 2000;342(20):1478-83.
- Russo D, Palmiero G, De Blasio AP, Balletta MM, Andreucci VE. Coronary artery calcification in patients with CRF not undergoing dialysis. Am J Kidney Dis. 2004;44(6):1024-30.
- Sigrist MK, Taal MW, Bungay P, McIntyre CW. Progressive vascular calcification over 2 years is associated with arterial stiffening and increased mortality in patients with stages 4 and 5 chronic kidney disease. Clin J Am Soc Nephrol. 2007;2(6):1241-8.
- Levey AS, Beto JA, Coronado BE, Eknoyan G, Foley RN, Kasiske BL, et al. Controlling the epidemic of cardiovascular disease in chronic renal disease: what do we know? What do we need to learn? Where do we go from here? National Kidney Foundation Task Force on Cardiovascular Disease. Am J Kidney Dis. 1998;32(5):853-906.
- Cozzolino M, Mazzaferro S, Pugliese F, Brancaccio D. Vascular calcification and uremia: what do we know? Am J Nephrol. 2008;28(2):339-46.
- McCullough PA, Sandberg KR, DumlerF, Yanez JE. Determinants of coronary vascular calcification in patients with chronic kidney disease and end-stage renal disease: a systematic review. J Nephrol. 2004;17(2):205-15.
- O’Neill WC, Lomashvili KA, Malluche HH, Faugere MC, Riser BL. Treatment with pyrophosphate inhibits uremic vascular calcification. Kidney Int. 2011;79(5):512-7.
- Goldsmith DJ, Covic A, Sambrook PA, Ackrill P. Vascular calcification in long-term haemodialysis patients in a single unit: a retrospective analysis. Nephron. 1997;77(1):37-43.
- Shanahan CM. Mechanisms of vascular calcification in CKD-evidence for premature ageing? Nat Rev Nephrol. 2013;9(11):661-70.
- Blacher J, Guerin AP, Pannier B, Marchais SJ, London GM. Arterial calcifications, arterial stiffness, and cardiovascular risk in end-stage renal disease. Hypertension. 2001;38(4):938-42.
- Ohtake T, Ishioka K, Honda K, Oka M, Maesato K, Mano T, et al. Impact of coronary artery calcification in hemodialysis patients: risk factors and associations with prognosis. Hemodial Int. 2010;14(2):218-25.
- London GM, Guérin AP, Marchais SJ, Métivier F, Pannier B, Adda H. Arterial media calcification in end-stage renal disease: impact on all-cause and cardiovascular mortality. Nephrol Dial Transplant. 2003;18(9):1731-40.
- Guérin AP, London GM, Marchais SJ, Metivier F. Arterial stiffening and vascular calcifications in end-stage renal disease. Nephrol Dial Transplant. 2000;15(7):1014-21.
- Adragao T, Pires A, Lucas C, Birne R, Magalhaes L, Gonçalves M, et al. A simple vascular calcification score predicts cardiovascular risk in haemodialysis patients. Nephrol Dial Transplant. 2004;19(6):1480-8.
- Raggi P, Bellasi A, Ferramosca E, Islam T, Muntner P, Block GA. Association of pulse wave velocity with vascular and valvular calcification in hemodialysis patients. Kidney Int. 2007;71(8):802-7.
- Kraus MA, Kalra PA, Hunter J, Menoyo J, Stankus N. The prevalence of vascular calcification in patients with end-stage renal disease on hemodialysis: a cross-sectional observational study. Ther Adv Chronic Dis. 2015;6(3):84-96.
- Okuno S, Ishimura E, Kitatani K, Fujino Y, Kohno K, Maeno Y, et al. Presence of abdominal aortic calcification is significantly associated with all-cause and cardiovascular mortality in maintenance hemodialysis patients. Am J Kidney Dis. 2007;49(3):417-25.
- Okuda K, Kobayashi S, Hayashi H, Ohtake H, Nakajima Y, Yoshida K, et al. Case-control study of calcification of the hepatic artery in chronic hemodialysis patients: comparison with the abdominal aorta and splenic artery. J Gastroenterol Hepatol. 2002;17(1):91-5.
- Jean G, Bresson E, Terrat JC, Vanel T, Hurot JM, Lorriaux C, et al. Peripheral vascular calcification in long-haemodialysis patients: associated factors and survival consequences. Nephrol Dial Transplant. 2009;24(3):948-55.
- Honkanen E, Kauppila L, Wikström B, Rensma PL, Krzesinski JM, Aasarod K, et al; CORD study group. Abdominal aortic calcification in dialysis patients: results of the CORD study. Nephrol Dial Transplant. 2008;23(12):4009-15.
- Kramer H, Toto R, Peshock R, Cooper R, Victor R. Association between chronic kidney disease and coronary artery calcification: the Dallas Heart Study. J Am Soc Nephrol. 2005;16(2):507-13.
- Raggi P, Boulay A, Chasan-Taber S, Amin N, Dillon M, Burke SK, et al. Cardiac calcification in adult hemodialysis patients. A link between end-stage renal disease and cardiovascular disease? J Am Coll Cardiol. 2002;39(4):695-701.
- Schwaiger JP, Neyer U, Sprenger-Mähr H, Kollerits B, Mündle M, Längle M, et al. A simple score predicts future cardiovascular events in an inception cohort of dialysis patients. Kidney Int. 2006;70(3):543-8.
- Shroff RC, McNair R, Figg N, Skepper JN, Schurgers L, Gupta A, et al. Dialysis accelerates medial vascular calcification in part by triggering smooth muscle cell apoptosis. Circulation. 2008;118(17):1748-57.
- London GM, Guérin AP, Verbeke FH, Pannier B, Boutouyrie P, Marchais SJ, et al. Mineral metabolism and arterial functions in end-stage renal disease: potential role of 25-hydroxyvitamin D deficiency. J Am Soc Nephrol. 2007;18(2):613-20.
- Chertow GM, Raggi P, Chasan-Taber S, Bommer J, Holzer H, Burke SK. Determinants of progressive vascular calcification in haemodialysis patients. Nephrol Dial Transplant. 2004;19(6):1489-96.
- Block GA, Spiegel DM, Ehrlich J, Mehta R, Lindbergh J, Dreisbach A, et al. Effects of sevelamer and calcium on coronary artery calcification in patients new to hemodialysis. Kidney Int. 2005;68(4):1815-24.
- Toussaint ND, Lau KK, Polkinghorne KR, Kerr PG. Attenuation of aortic calcification with lanthanum carbonate versus calcium-based phosphate binders in haemodialysis: a pilot randomized controlled trial. Nephrology (Carlton). 2011;16(3):290-8.
- Qunibi W, Moustafa M, Muenz LR, He DY, Kessler PD, Diaz-Buxo JA, et al; CARE-2 Investigators. A 1-year randomized trial of calcium acetate versus sevelamer on progression of coronary artery calcification in hemodialysis patients with comparable lipid control: the Calcium Acetate Renagel Evaluation-2 (CARE-2) study. Am J Kidney Dis. 2008;51(6):952-65.
- Zhang Q, Li M, Lu Y, Li H, Gu Y, Hao C, et al. Meta-analysis comparing sevelamer and calcium-based phosphate binders on cardiovascular calcification in hemodialysis patients. Nephron Clin Pract. 2010;115(4):c259-67.
- Wilson PW, Kauppila LI, O’Donnell CJ, Kiel DP, Hannan M, Polak JM, et al. Abdominal aortic calcific deposits are an important predictor of vascular morbidity and mortality. Circulation. 2001;103(11):1529-34.
- Shantouf RS, Budoff MJ, Ahmadi N, Ghaffari A, Flores F, Gopal A, et al. Total and individual coronary artery calcium scores as independent predictors of mortality in hemodialysis patients. Am J Nephrol. 2010;31(5):419-25.
- Shimoyama Y, Tsuruta Y, Niwa T. Coronary artery calcification score is associated with mortality in Japanese hemodialysis patients. J Ren Nutr. 2012;22(1):139-42.
- Wilkieson TJ, Rahman MO, Gangji AS, Voss M, Ingram AJ, Ranganath N, et al. Coronary artery calcification, cardiovascular events, and death: a prospective cohort study of incident patients on hemodialysis. Can J Kidney Health Dis. 2015;2:29.
- Block GA, Raggi P, Bellasi A, Kooienga L, Spiegel DM. Mortality effect of coronary calcification and phosphate binder choice in incident hemodialysis patients. Kidney Int. 2007;71(5):438-41.
- Noordzij M, Cranenburg EM, Engelsman LF, Hermans MM, Boeschoten EW, Brandenburg VM, et al; NECOSAD Study Group. Progression of aortic calcification is associated with disorders of mineral metabolism and mortality in chronic dialysis patients. Nephrol Dial Transplant. 2011;26(5):1662-9.
- Inoue T, Ogawa T, Ishida H, Ando Y, Nitta K. Aortic arch calcification evaluated on chest X-ray is a strong independent predictor of cardiovascular events in chronic hemodialysis patients. Heart Vessels. 2012;27(2):135-42.
- Adragao T, Pires A, Branco P, Castro R, Oliveira A, Nogueira C, et al. Ankle—brachial index, vascular calcifications and mortality in dialysis patients. Nephrol Dial Transplant. 2012;27(1):318-25.
- Ohtake T, Oka M, Ikee R, Mochida Y, Ishioka K, Moriya H, et al. Impact of lower limbs’ arterial calcification on the prevalence and severity of PAD in patients on hemodialysis. J Vasc Surg. 2011;53(3):676-83.
|