https://doi.org/10.59793/ijcp.v34i2.456
Abstract
Pleomorphic adenoma is the most common salivary gland tumor accounting for 80% of all major salivary gland tumors. It is a benign salivary gland neoplasm that constitutes 3% to 10% of the neoplasms in the head and neck region.1 Salivary gland neoplasms represents less than 1% of all tumors. This article is being showcased as a special case due to the fact it was done at a Taluk Hospital and also because ENT and oromaxillofacial surgeons were involved during the surgery.
Keywords: Pleomorphic adenoma, palate, minor salivary gland
Pleomorphic adenoma is a benign mixed tumor composed of epithelial and myoepithelial cells arranged with various morphological patterns; it is demarcated from the surrounding tissues by a fibrous capsule. Pleomorphic adenoma commonly affects the parotid gland and palate is the most common site wherein minor salivary glands are affected.
Other intraoral sites that could be involved are lip, buccal mucosa, floor of the mouth, tongue, tonsil, pharynx and retromolar area. In the palate region, it commonly affects the posterolateral surface of the hard palate.2
Surgical excision of the tumor is the only modality of treatment.
CASE REPORT
A 50-year-old lady presented to the ENT OPD with a mass in the oral cavity, which she had noticed since 6 months. The mass slowly grew to the present size and was painless. There was no history of stridor, dysphagia or chewing difficulties due to the swelling.
On examination, the growth measured 2.5 × 2.5 cm in size. It appeared smooth with no ulcerations or bleeding points, etc. thus ruling out a malignant growth (Fig. 1).

Figure 1. Hard palate growth.
On palpation, the swelling was unilocular, nontender, firm, immobile with a well-defined margin. The mucosa over the growth was stretched and lymph nodes of the neck appeared normal.
The patient was then counseled for surgery after getting a plain computed tomography (CT) scan (Fig. 2) to rule out any erosion of the palate. The scan also revealed a soft tissue mass in the hard palate region.
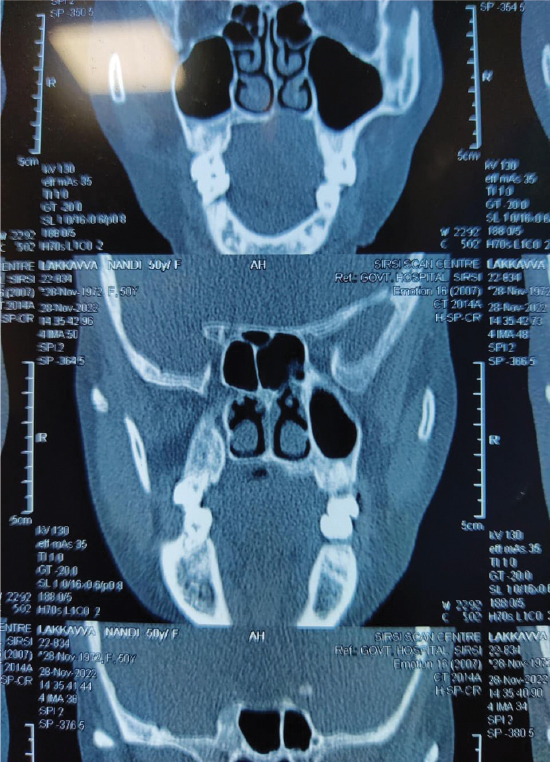
Figure 2. CT scan film of the patient shwoing the hard palate region.
Prior to the surgery, as an OPD procedure, alginate impression was taken by the oromaxillofacial surgeon and a 3D cast was made using type 2 dental stone to fabricate an obturator post surgery.
This obturator was used to protecting the surgical wound from infection in the postoperative period and prevent dehiscence as the surgical site was devoid of any soft tissue graft.
Routine blood investigations were also done and after obtaining physician’s fitness the patient underwent surgical excision of the growth under general anesthesia.
The growth was excised in total after ensuring that there were no residual extracapsular projections, which could lead to a further recurrence. The defect was sutured and the prefabricated obturator with an antiseptic dressing comprising of a povidone-iodine gauze was kept in situ, with a nasogastric tube inserted in order to ensure no contamination of the wound occurred once feeding was started (Fig. 3).

Figure 3. Intraoperative photo of the growth excised with bite block in situ.
The excised mass was sent for histopathological examination (Figs. 4-6).
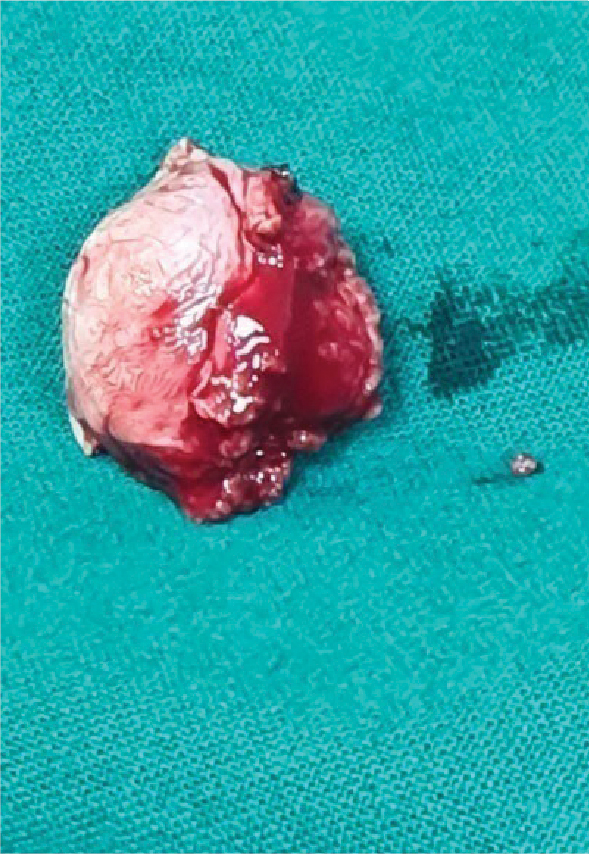
Figure 4. The palatal mass excised in total.

Figure 5. Pathological specimen of the growth.

Figure 6. Cut section of the specimen.
The microscopic picture showed epithelial and stromal components (Fig. 7). The epithelial component had epithelial cells arranged in tubules, acini, chords; cystic spaces were also seen. The stromal component had myxoid and hyalinized areas with spindle cells which goes in favor of pleomorphic adenoma.
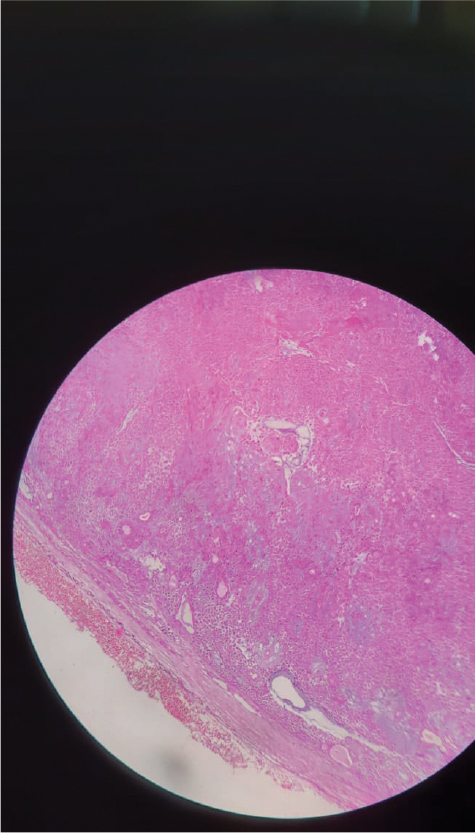
Figure 7. Microscopic picture of the specimen.
On the 5th postoperative day, the patient was discharged with oral antibiotics and instructions regarding oral hygiene and advised to follow-up after a week to the ENT OPD (Fig. 8).

Figure 8. One week post-op picture with healthy granulation tissue.
The patient has been followed up for 3 months, has excellent healing with no complaints and no signs of recurrence.
DISCUSSION
Pleomorphic adenomas are derived from a mixture of ductal and myoepithelial elements.3 They are the commonest benign salivary gland tumors (80%) as well as the commonest benign tumor of the minor salivary gland. It occurs most frequently on the palatal area (73%),4 commonly seen on the posterolateral aspect of the palate. Females are more affected than males with a ratio of 2:1; commonly seen in the 40 to 50 years age group.
It is detected and treated earlier than tumors of the major salivary gland.5 If the overlaying mucosa is ulcerated, then malignancy should be suspected.
CT scan is an important diagnostic tool in such tumors as it helps to determine the extent of the lesion. Since it is a benign tumor, it is less likely to cause invasion of the bone; however, it may cause bone resorption due to pressure effect.6
Tumors of the hard palate are usually excised down to the periosteum including the overlying mucosa with 1 cm margin at the periphery. Pleomorphic adenoma does not recur after adequate surgical excision. Reasons for recurrence include incomplete excision of the tumor in total, seeding or cutting through the microscopic extracapsular projection.6
CONCLUSION
The patient recovered well after the surgery, and on the 5th postoperative day, she was discharged with oral antibiotics and instructions for oral hygiene. Follow-up examinations showed excellent healing with no signs of recurrence.
Pleomorphic adenomas are derived from a mixture of ductal and myoepithelial elements and are the most common benign salivary gland tumors. They frequently occur in the palatal area, with females being more affected than males. Complete surgical excision is the treatment of choice, and recurrence is rare if the tumor is adequately removed.
This case highlights the successful management of a pleomorphic adenoma in the hard palate, emphasizing the importance of multidisciplinary involvement and thorough surgical excision for optimal patient outcomes.
REFERENCES
- Pons Vicente O, Almendros Marqués N, Berini Aytés L, Gay Escoda C. Minor salivary gland tumors: a clinicopathological study of 18 cases. Med Oral Patol Oral Cir Bucal. 2008;13(9):E582-8.
- Moghe S, Pillai AK,Prabhu S, Nahar S, Kartika IK. Pleomorphic adenoma of the palate: report of a case. Int J Sci Stud. 2014;2(1):54-6.
- Chau MN, Radden BG. A clinical-pathological study of 53 intraoral pleomorphic adenomas. Int J Oral Maxillofac Surg. 1989;18(3):158-62.
- Toida M, Shimokawa K, Makita H, Kato K, Kobayashi A, Kusunoki Y, et al. Intraoral minor salivary gland tumors: a clinicopathological study of 82 cases. Int J Oral Maxillofac Surg. 2005;34(5):528-32.
- Shafer WG, Hine MK. Levy BM. Textbook of Oral Pathology. 4th Edition, West Washington Square, WB Saunders Company, Philadelphia; 1983.
- Daniels JS, Ali I, Al Bakri IM, Sumangala B. Pleomorphic adenoma of the palate in children and adolescents: a report of 2 cases and review of the literature. J Oral Maxillofac Surg. 2007;65(3):541-9.