Dual left circumflex (LCx) arteries represent a very rare congenital anomaly with only few reported cases in literature. Herein, we present a case of dual LCx arteries originating from the left main coronary artery (LMCA) and right coronary artery (RCA), respectively.
A 40-year-old male presented in emergency department with complaint of chest pain. On examination, his pulse rate was 90 beats/min and blood pressure 120/70 mmHg. Electrocardiogram (ECG) showed ST depression in inferior leads. Cardiac markers creatine phosphokinase-MB and troponin I was within normal limits.
Echocardiography revealed hypokinetic inferolateral wall. Elective coronary angiography was then planned, which showed twin LCx arteries: one originating from LMCA and the other from the proximal RCA (Figs. 1 and 2). Patient was discharged on optimal medical therapy and he remained asymptomatic in follow-up period.
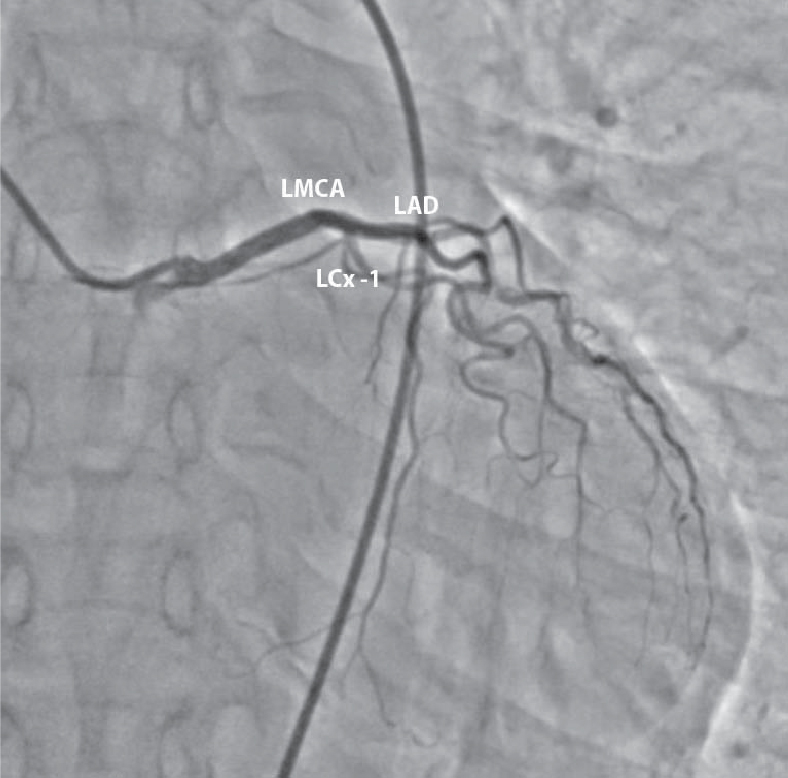
Figure 1. Left coronary angiogram showing small, left circumflex artery (LCx-1) arising from left main coronary artery (LMCA).
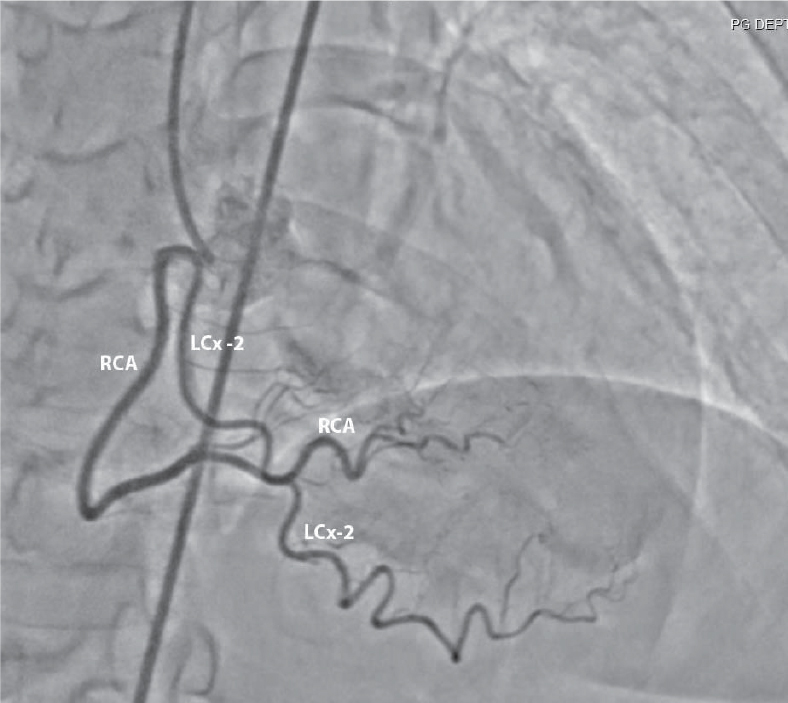
Figure 2. Right coronary angiogram showing second left circumflex artery (LCx-2) arising from right coronary artery (RCA).
Coronary anomalies are rare. The most frequently found anomalies include a LCx artery with a separate origin of the left anterior descending (LAD), followed by a LCx artery arising from the right sinus of Valsalva or the RCA.1 Only a few cases of twin circumflex arteries originating from both left and right coronary systems have been reported in the literature.2-4 It may cause chest pain, heart failure, arrhythmia and sudden death as a consequence of the repeated compression of the anomalous artery by a dilated aortic root or of slit-like ostia or of unusual angling as a result of the retroaortic course of the LCx.5
The clinical significance of this anomaly may be important in patients undergoing coronary intervention or cardiac surgery. It is important to inform the surgeons so as to accidentally avoid cross-clamping or transecting the artery during surgery.
REFERENCES
- Angelini P, Villason S, Chan AV, Diez RJG. Normal and anomalous coronary arteries in humans. In: Angelini P (Ed.). Coronary Artery Anomalies: A Comprehensive Approach. Philadelphia, PA: Lippincott Williams & Wilkins; 1999. pp. 27-79.
- Karabay KO, Uysal E, Bagirtan B, Vural M. A case of twin circumflex arteries associated with acute myocardial infarction. Turk Kardiyol Dern Ars. 2010;38(7):496-8.
- Uluçay A. A case of twin circumflex arteries associated with acute myocardial infarction. Turk Kardiyol Dern Ars. 2011;39(4):348; author reply 349-50.
- Uguz B, Tiryakioglu SK, Öztas S, Karakus A. A very rare coronary artery anomaly: twin circumflex arteries associated with acute coronary syndrome - two cases report. Arch Clin Cases. 2021;7(2):22-7.
- Aydin M, Ozeren A, Peksoy I, Cabuk M, Bilge M, Dursun A, et al. Myocardial ischemia caused by a coronary anomaly: left circumflex coronary artery arising from right sinus of valsalva. Tex Heart Inst J. 2004;31(3):273-5.