https://doi.org/10.59793/ijcp.v34i5.675
Abstract
A retrospective observational study was undertaken to evaluate the clinical profile of recurrent urinary tract infections (UTIs) in a tertiary care hospital. Patients <18 years, kidney-transplant recipients, those on immunosuppressive agents and pregnant patients were excluded. Patients with ³2 episodes of culture positive UTIs were included. Demographic details, investigations and treatment were recorded. Out of total 48 patients, 18 were female and 30 male. The common manifestations were acute pyelonephritis (52%), emphysematous pyelonephritis (20%) and cystitis (25%). Extended-spectrum beta-lactamase (ESBL)-producing Escherichia coli (48%) was the most frequent organism isolated followed by Klebsiella spp. (29%) and Pseudomonas spp. (23%). Recurrent episodes of UTI with same organisms were noted in 62% patients. Death occurred in 12.5% patients due to septic shock. Renal calculi (24%) and double J (DJ) stent placement (30%) were associated with recurrent UTIs, though this was not statistically significant. Resistance to higher antibiotics (colistin, carbapenems, piperacillin-tazobactam, cefoperazone-sulbactam, third-generation cephalosporins) (65.4%, r = 0.81), diabetes (62.5%, r = 0.79), urological procedure (39.5%, r = 0.68), prior hospitalization (75%, r = 0.84), history of UTI prior to the study period (44%, r = 0.72) and need for per urethral catheter (PUC) beyond 7 days (35%, r = 0.74) had significant correlation with recurrent UTIs.
Keywords: Recurrent urinary tract infections, urinary tract infections, multidrug-resistant microbes
Urinary tract infections (UTIs) are one of the most frequent community-associated and health care-derived infections that drive antibiotic usage and hospitalizations around the world. The prevalence of UTI in the general population is 11%, while elderly women (age >65 years) exhibit a higher prevalence at 20%.1 Uropathogenic Escherichia coli (E. coli) (UPEC) is the dominant infectious agent in both uncomplicated and complicated UTIs. Enterococcus spp. and Candida spp. are substantially more common in complicated infections, while Staphylococcus saprophyticus (S. saprophyticus) is rare.1
Recurrent UTI is described ≥2 infections in 6 months or ≥3 infections in 1 year.1 From the clinical perspective, the second episode of UTI can be considered as a recurrence and requires a diligent approach to diagnosis and management.
In this retrospective observational study, we aimed to evaluate the clinical spectrum of recurrent UTIs in a tertiary care hospital and identify etiological factors contributing to this entity.
The objectives were to also study the microbiological spectrum and antimicrobial resistance patterns of organisms causing recurrent UTIs and evaluate the associated significant risk factors.
MATERIALS AND METHODS
A retrospective observational single-center study in a tertiary care hospital in Mumbai, India was conducted from 1st January 2021 to 31st December 2021. Indoor patients aged >18 years, with ≥2 episodes of culture-positive UTIs, were included. Patients <18 years, kidney-transplant recipients, those on immunosuppressive agents and pregnant patients were excluded. Demographic details, clinical symptoms, signs, drug history including use of sodium-glucose co-transporter type 2 (SGLT2) inhibitors, radiological and laboratory data including urine and blood cultures, of all patients were recorded in the Case Record Form. The details of treatment including urological interventions received and outcomes in hospital were noted. Clinical history and details of treatment of prior hospitalization with UTI were also recorded. Bacterial isolates from urine and blood culture were identified by biochemical profiling using VITEK-2 System, an automated microbiology bacterial identification and antimicrobial susceptibility system. The extended-spectrum beta-lactamase (ESBL) test was done using VITEK-2 ESBL test. Pearson correlation coefficient was used as a statistical method to determine association.
The study was conducted with approval from Institutional Ethics Committee.
RESULTS
Forty-eight patients satisfied the inclusion criteria; of these, 37.5% were female and 62.5% were male. Their mean age was 57.8 + 11.2 years. Fever (79%), dysuria (60%) and flank pain (50%) were the most common symptoms. The common manifestations of UTI were acute pyelonephritis (52%), emphysematous pyelonephritis (20%) and cystitis (25%). Recurrent episodes of UTI with same organism were noted in 62% patients and 12.5% patients died due to septic shock.
ESBL E. coli (48%) was the most frequent organism isolated followed by Klebsiella spp. (29%) and Pseudomonas spp. (23%) (Fig. 1). The antimicrobial resistance pattern was as follows: colistin (8%), carbapenems (72%), piperacillin/tazobactam (80%), cefoperazone/sulbactam (75%), aminoglycosides (72%), fluoroquinolones (80%), third-generation cephalosporins (92%) and penicillins (95%) (Fig. 2).
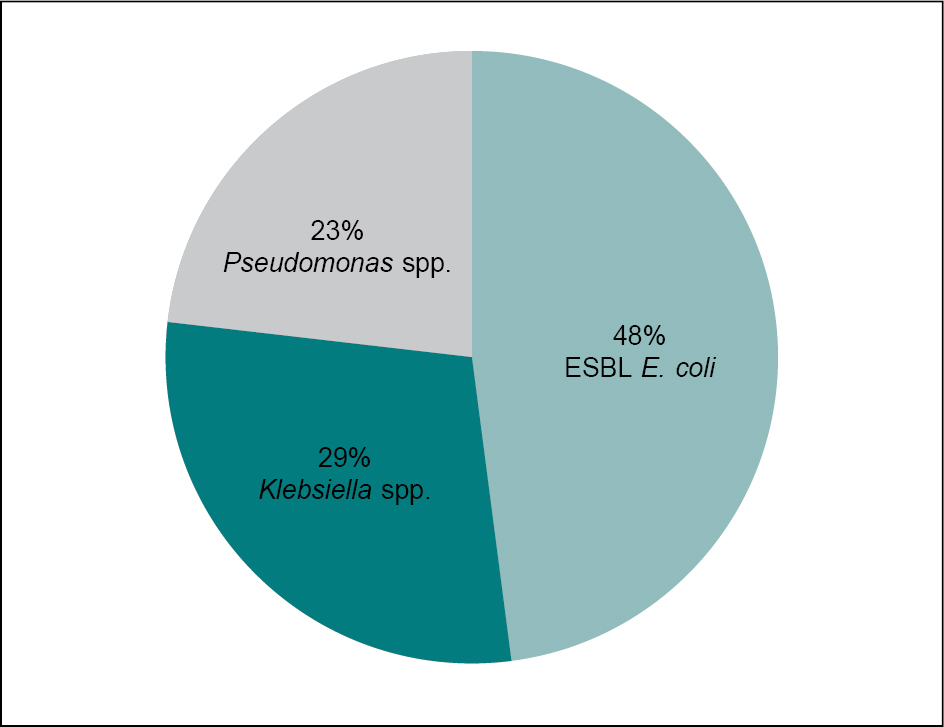
Figure 1. Microbiological spectrum of recurrent UTI.
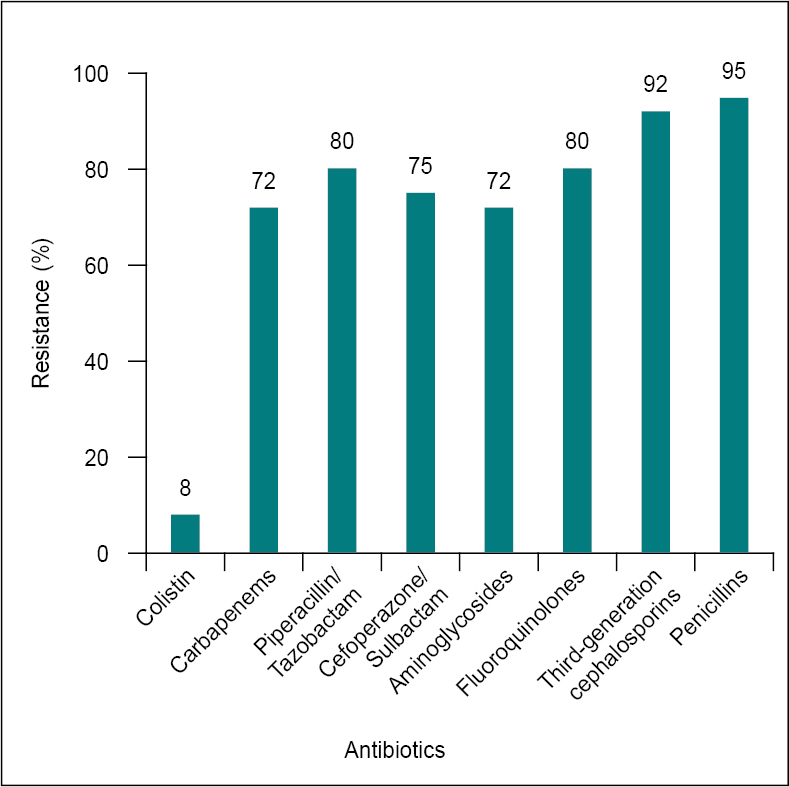
Figure 2. Antimicrobial resistance pattern.
Renal calculi (24%), DJ stent placement (30%), use of SGLT2 inhibitors (8.3%) did not correlate statistically with recurrent UTI; however, resistance to higher antibiotics (64.5%, r = 0.81), diabetes (62.5%, r = 0.79), urological procedure (39.5%, r = 0.68), prior hospitalization (75%, r = 0.84), history of UTI prior to the study period (44%, r = 0.72) and need for per urethral catheter (PUC) beyond 7 days (35%, r = 0.74) had statistically significant correlation with recurrent UTIs.
Figure 3 shows the risk factors that had statistically significant association with recurrent UTIs.
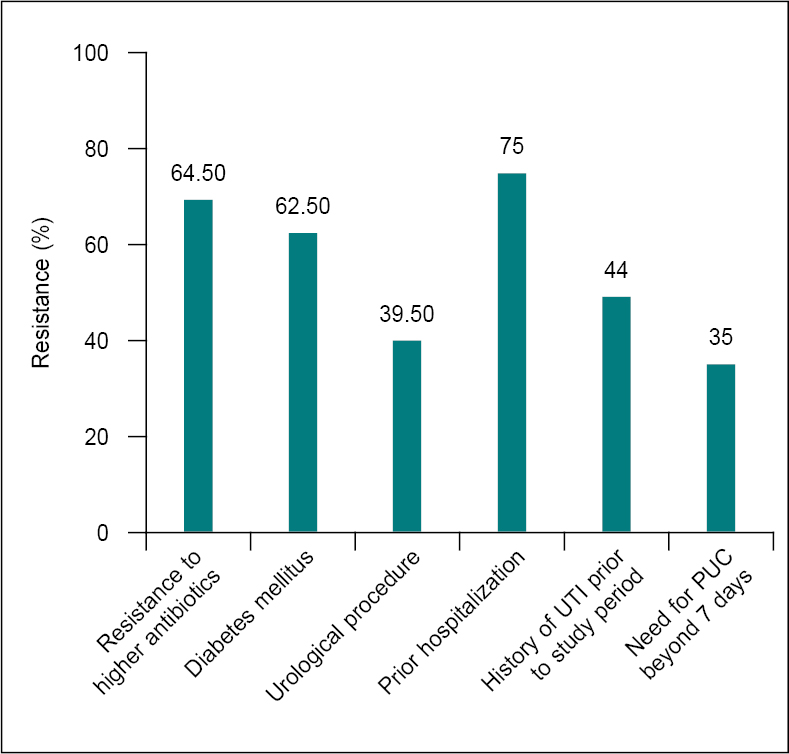
Figure 3. Significant risk factors associated with recurrent UTIs.
DISCUSSION
Urinary tract infections are among the most common infections in all age groups, which can have a wide presentation from simple cystitis to very severe pyelonephritis. Recurrent UTIs, as one of the most common problems in nephrology and urological clinics, significantly increase health care costs and bear a negative impact on the patients’ quality of life. The incidence of recurrent UTIs may be as high as 44%.1 After a first episode of an uncomplicated UTI, at least 1 second episode will occur in 27% of women in the next 6 to 12 months.2 The clinical presentation and pathogenesis of recurrent UTIs is similar to sporadic UTI.
The pathogenesis of recurrent UTI might include two mechanisms-bacterial factors and deficiency in host defense mechanism.
The bacterial factors that contribute to recurrent UTIs are described below.
Gastrointestinal tract functions as a reservoir for uropathogens, which are repeatedly reintroduced into the urinary tract via contamination of the periurethral surface and subsequent retrograde ascension.3
Strain-specific bacterial virulence factors such as flagella/pili, adhesins, extracellular polysaccharides, lipopolysaccharides, toxins, ureases, proteases and iron-scavenging siderophores, biofilm formation may also have a role in pathogenesis of recurrent UTIs.
A subpopulation of bacterial cells (“persistors”) in the biofilm, are known to reversibly reduce their metabolic activity, adopting a dormant state that can evade host defenses as well as treatments that target active metabolic pathways or activities such as cell division.4
Bacterial resistance and resilience: The overuse of antibiotics has led to emergence of strains with specific genetic traits allowing them to survive and proliferate in the presence of a single or even a class of antimicrobial compounds.5,6
Mean age of the study group was 57.8 ± 11.2 years with a relatively younger and predominantly male (62.5%) population, contrary to other studies that had an older and predominantly female population.1,7 Fever (79%), dysuria (60%) and flank pain (50%) were the most common symptoms similar to the presentation in the study by Hase et al.8
The most frequent organism isolated in our study was ESBL E. coli (48%) followed by Klebsiella spp. (29%) and Pseudomonas spp. (23%). In a recent study of 477 patients assessing risk factors and efficacy of low-dose prophylactic antibiotic therapy in adult patients with recurrent UTIs, the most common uropathogens isolated in urine culture were E. coli (49%), Klebsiella pneumoniae (21%), Enterococcus faecalis (9.2%).9 Multidrug-resistant (MDR) organisms are now frequently implicated in recurrent UTIs.
Figure 4 and Table 1 explains the mechanisms for multidrug resistance and describes the coding genes, corresponding enzymes and implicatory organisms in drug-resistant UTIs.
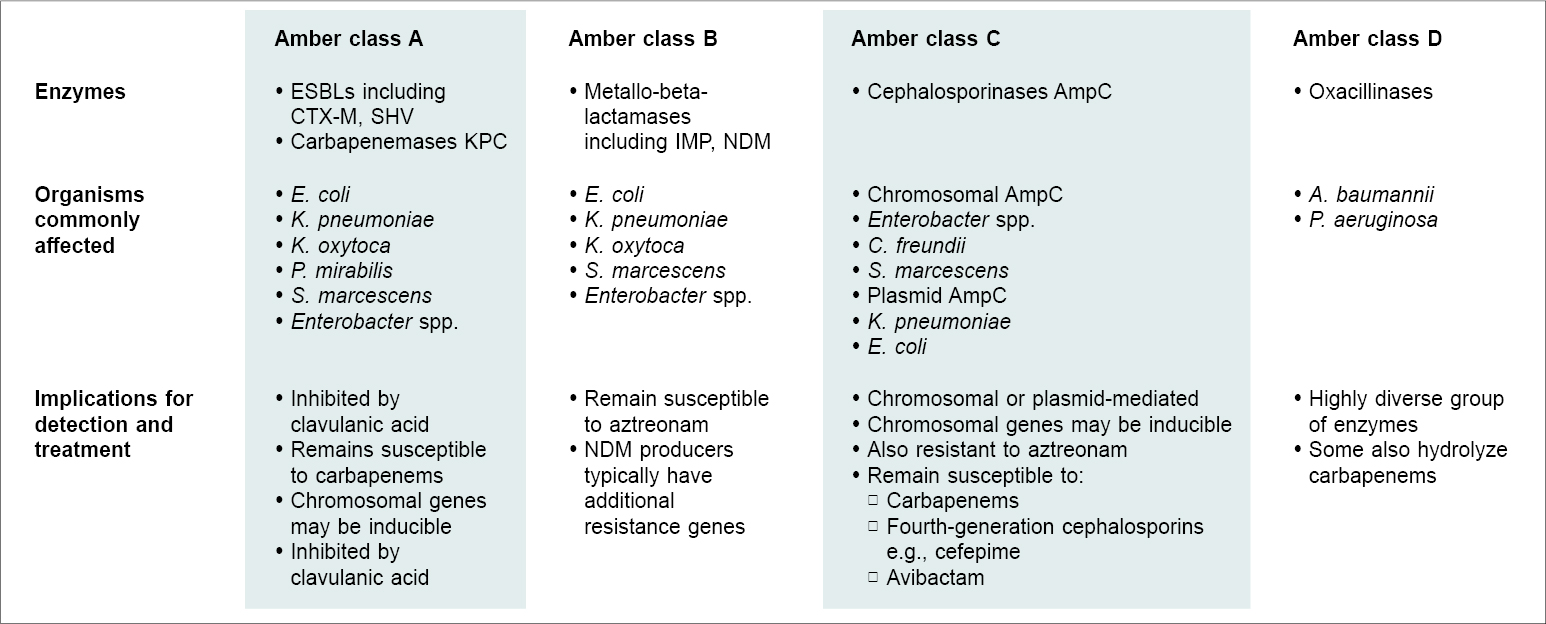
Figure 4. Amber classification of selected beta-lactamases.10
ESBL = Extended-spectrum beta-lactamases; CTX-M = Cefotaxime-Munich; SHV = Sulfhydryl variable; KPC = Klebsiella pneumoniae carbapenemase; IMP = Imipenem; NDM = New Delhi metallo-beta-lactamase; AmpC = Ampicillinase C.
Adapted from: Mahony M, McMullan B, Brown J, Kennedy SE. Multidrug-resistant organisms in urinary tract infections in children. Pediatr Nephrol. 2020;35(9):1563-73.
|
Table 1. Mechanisms of Resistance of Other Antibiotics10
|
|
Antibiotic class
|
Mechanism of resistance
|
Organisms
|
|
Aminoglycosides
|
Target site mutation - production of 16S rRNA methylases
|
E. coli
K. pneumoniae
Acinetobacter spp.
|
|
Quinolones
|
Drug modification - production of aminoglycoside-modifying enzymes
Phosphotransferases (APH)
Acetyltransferases (AAC)
Nucleotidyltransferases (ANT)
Target site mutation - DNA gyrase and topoisomerase IV
|
E. coli
K. pneumoniae
A. baumannii
P. aeruginosa
E. coli
Klebsiella spp.
P. aeruginosa
|
|
Trimethoprim or trimethoprim-sulfamethoxazole
|
Pentapeptide repeats - Qnr
Overproduction of enzymes
Dihydropteroate synthase (DHPS)
Dihydrofolate reductase (DHFS)
|
E. coli
Klebsiella spp.
E. coli
|
Adapted from: Mahony M, McMullan B, Brown J, Kennedy SE. Multidrug-resistant organisms in urinary tract infections in children. Pediatr Nephrol. 2020;35(9):1563-73.
ESBLs are variants of beta-lactamases that confer resistance to the extended-spectrum cephalosporin antibiotics such as cefotaxime, monobactams and aztreonam. The reason for this resistance is that ESBLs are encoded by plasmids, which also carry resistance genes for other antibiotics.6 In a cross-sectional study of 427 patients assessing the prevalence and risk factors of ESBL-producing uropathogens, the prevalence was 38.4% with E. coli being the most frequent uropathogen.11 Patients with recurrent UTI had 5 times higher relative risk of having ESBL-producing uropathogens (odds ratio [OR], 4.7) followed by previous antibiotic use (OR 3.07), hemodialysis (OR 2.92), chronic kidney disease (OR 2.69) and diabetes mellitus (OR 1.87).11
In our study, E. coli, Klebsiella and Pseudomonas spp. showed resistance to carbapenems (72%), piperacillin/tazobactam (80%), cefoperazone/sulbactam (75%), aminoglycosides (72%), fluoroquinolones (80%), third-generation cephalosporins (92%) and penicillins (95%). Resistance to higher antibiotics was seen in 64.5% (r = 0.81) of the study population.
In a study assessing antibiotic resistance of uropathogens in hospitalized patients, K. pneumoniae were resistant to amoxicillin + clavulanic acid (75.0%), piperacillin + tazobactam (76.2%), cefotaxime (76.2%), cefuroxime (81.0%), ciprofloxacin (81.0%) and trimethoprim + sulfamethoxazole (81.0%). Carbapenems were effective against all E. coli and Proteus mirabilis. Some K. pneumoniae isolates (13.6%), two from internal and one from nephrology wards, produced metallo-beta-lactamases (MBLs). E. coli (22.6%), K. pneumoniae (81.8%) and all Enterococcus faecium were MDR organisms. Some E. coli (26.2%), K. pneumoniae (63.6%) and P. mirabilis (14.3%) isolates produced ESBL. Vancomycin-resistant E. faecium was also found.12
Our study reiterates the escalating antimicrobial resistance in this region and the difficulty in the choice of empiric therapy. It also underlines the importance of sending appropriate cultures before antibiotic initiation to aid in better outcome.
Recent rise in the use of SGLT2 inhibitors has been met with a surge in the incidence of genitourinary tract infections as demonstrated in a retrospective cohort study of 253 diabetics on SGLT2 inhibitors, where the 3- and 6-month incidences of UTIs were 1.98% and 13.57%, respectively.13 In our study, use of SGLT2 inhibitors (8.3%) was associated with recurrent UTI though this was not statistically significant.
Similarly, renal calculi (24%) and DJ stent placement (30%) were associated with recurrent UTI though not statistically significant. Diabetics comprised 62.5% of our study group that was higher as compared to the cohort studied by Nabi14 (39.6%).
In our study, resistance to higher antibiotics (64.5%, r = 0.81), diabetes (62.5 %, r = 0.79), urological procedure (39.5%, r = 0.68), prior hospitalization (75%, r = 0.84), history of UTI prior to the study period (44%, r = 0.72) and need for PUC beyond 7 days (35%, r = 0.74) had significant correlation with recurrent UTI. In a study assessing risk factors and efficacy of low-dose prophylactic antibiotics in 250 adult patients with recurrent UTIs, diabetes mellitus, chronic renal disease, use of immunosuppressive drugs, renal transplant, any form of urinary tract catheterization, immobilization, neurogenic bladder, history of urinary incontinence and urological procedures showed statistically significant association.9
A limitation of our study is that it only included patients who had to be hospitalized in a tertiary care hospital for recurrent UTI. This precludes community-acquired UTI, which may be recurrent but does not need hospitalization. Additionally, a susceptible population of kidney transplant recipients and those on immunosuppressive medication were not included in the study.
CONCLUSION
Our study thus highlights the constantly growing epidemic of recurrent UTIs and associated risk factors even in those subgroups of patients who ordinarily are not susceptible to recurrent UTI. Resistance to higher antibiotics, urological interventions, diabetes, prior hospitalization, history of UTI prior to study period, need for PUC beyond 7 days contribute to the rising incidence of recurrent UTIs. The associated morbidity takes a heavy toll on the patient’s well-being and the health infrastructure. Appropriate and pre-emptive redressal of the underlying etiological factors could assist in reducing the incidence of recurrent UTI. Precise knowledge of the antibiotic resistance pattern of the local microflora and uropathogens is essential to curb the menace of MDR UTI. Thus, close follow-up of patients with risk factors after their first episode of UTI, adoption of antimicrobial and nonantimicrobial preventive strategies and antibiotic stewardship is the need of the hour before this epidemic reaches alarming proportions.
REFERENCES
- Medina M, Castillo-Pino E. An introduction to the epidemiology and burden of urinary tract infections. Ther Adv Urol. 2019;11:1756287219832172.
- Jung C, Brubaker L. The etiology and management of recurrent urinary tract infections in postmenopausal women. Climacteric. 2019;22(3):242-9.
- Jones-Freeman B, Chonwerawong M, Marcelino VR, Deshpande AV, Forster SC, Starkey MR. The microbiome and host mucosal interactions in urinary tract diseases. Mucosal Immunol. 2021;14(4):779-92.
- Murray BO, Flores C, Williams C, Flusberg DA, Marr EE, Kwiatkowska KM, et al. Recurrent urinary tract infection: a mystery in search of better model systems. Front Cell Infect Microbiol. 2021;11:691210.
- Mattoo TK, Asmar BI. Annotations on emerging concerns about antibiotic-resistant urinary tract infection. Pediatrics. 2020;145(2):e20193512.
- Malik B, Bhattacharyya S. Antibiotic drug-resistance as a complex system driven by socio-economic growth and antibiotic misuse. Sci Rep. 2019;9(1):9788.
- Geerlings SE. Clinical presentations and epidemiology of urinary tract infections. Microbiol Spectr. 2016;4(5):4-5.
- Hase AN, Bansal SB, Gadde AB, Nandwani A. Microbiological spectrum, and outcomes of acute pyelonephritis in north Indian population. Saudi J Kidney Dis Transpl. 2021;32(1):209-17.
- Alghoraibi H, Asidan A, Aljawaied R, Almukhayzim R, Alsaydan A, Alamer E, et al. Recurrent urinary tract infection in adult patients, risk factors, and efficacy of low dose prophylactic antibiotics therapy. J Epidemiol Glob Health. 2023;13(2):200-11.
- Mahony M, McMullan B, Brown J, Kennedy SE. Multidrug-resistant organisms in urinary tract infections in children. Pediatr Nephrol. 2020;35(9):1563-73.
- Abu Taha A, Shtawi A, Jaradat A, Dawabsheh Y. Prevalence and risk factors of extended spectrum beta-lactamase-producing uropathogens among UTI patients in the governmental hospitals of North West Bank: a cross-sectional study. J Infect Dis Preve Med. 2018;6(183):2.
- Kot B, Gruzewska A, Szweda P, Wicha J, Parulska U. Antibiotic resistance of uropathogens isolated from patients hospitalized in district hospital in Central Poland in 2020. Antibiotics (Basel). 2021;10(4):447.
- Caro MCK, Cunanan EC, Kho SA. Incidence and factors associated with genitourinary infections among type 2 diabetes patients on SGLT2 inhibitors: a single retrospective cohort study. Diabet Epidemiol Manag. 2022;7:100082.
- Nabi T. Clinical profile and risk factors of recurrent urinary tract infection in patients with type 2 diabetes. Int J Acad Med. 2020;6(4):301-8.