Published in IJCP
December 2023
Case Report
An Unusual Case of Liver Abscess Caused by Trematodes
December 11, 2023 | Chinnasami Vijaikumar, P Ruba
General Medicine Hepatology
Abstract
Liver abscess caused by trematodes is considered highly unusual. Here we present a case of an elderly female with no known comorbidities, who presented with fever and right upper quadrant pain. Upon evaluation, she was found to have features of liver abscess on abdominal ultrasound and 640-slice computed tomography (CT) of the abdomen. Ultrasound-guided needle biopsy of the liver showed features of trematode. Patient was treated with oral nitazoxanide. Patient’s fever and abdominal pain subsided after the treatment.
Keywords: Liver flukes, rare, right upper quadrant pain, ultrasound-guided needle biopsy
Liver abscess is a pus-filled collection in the liver. It is one of the most common forms of visceral abscess. It can develop either from an intra-abdominal infective source disseminated through portal circulation or following an injury. Majority of them are caused by bacteria or amoeba while rarely caused by fungi and parasites.1 Approximately 91 species of trematodes or flatworms, called flukes are known to affect humans worldwide.2 Rarely, liver abscess formation may occur secondary to hepatic inflammation or cholangitis. Some authors argue that tolerance instead of the immunity is the preferred immunological response of liver, which offers a favorable environment for the parasites.3 The common liver flukes include Fasciola hepatica, Fasciola gigantica, Opisthorchis viverrini, Opisthorchis felineus and Clonorchis sinensis. Liver abscess caused by trematodes is considered highly unusual. A definitive diagnosis of trematode-induced liver abscess can be made based on detection of eggs in stool, tissue samples or based on serological tests. Nonspecific and asymptomatic clinical presentation often hampers the diagnosis.3 Cholangiocarcinoma is the most dreaded complication of C. sinensis and O. viverrini, which needs early evaluation and treatment.4
CASE REPORT
A 72-year-old female presented with chief complaints of intermittent fever and generalized weakness for 2 years. She had a history of open drainage, debridement and peritoneal lavage for a liver abscess (involving the 7th segment) 2 years back. She also had right-sided abdominal pain and loss of appetite since then. She denied any history of abdominal distension, jaundice, loss of weight or bowel and bladder disturbances.
On examination, patient was conscious and oriented. Her vital data were within normal limits. Systemic examination revealed tenderness in the right hypochondrium. Her baseline blood investigations showed anemia (Table 1).1 Chest X-ray was normal. Ultrasonogram (USG) of the abdomen showed mild hepatomegaly with a cystic space-occupying lesion.
|
Table 1. Baseline Parameters of the Patient
|
|
Parameters
|
Patient’s value
|
Normal value
|
|
Hemoglobin
|
10.6 g/dL
|
12-16 g/dL
|
|
White cell count
|
5.81 × 10/mm3
|
4-11 × 10/mm3
|
|
Neutrophils
|
62
|
40-80
|
|
Lymphocytes
|
22
|
20-40
|
|
Eosinophils
|
9
|
1-6
|
|
Monocytes
|
6
|
2-10
|
|
Platelet count
|
155 × 10/mm3
|
150-450 × 10/mm3
|
|
Serum creatinine
|
0.5 mg/dL
|
0.7-1.3 mg/ dL
|
|
Alanine transaminase (ALT)
|
34 U/L
|
<34 U/L
|
|
Aspartate transaminase (AST)
|
38 U/L
|
<31 U/L
|
|
Alkaline phosphatase (ALP)
|
97 U/L
|
<141 U/L
|
|
Gamma-glutamyl transpeptidase (GGTP)
|
17 U/L
|
<38 U/L
|
|
Total bilirubin
|
1.3 mg/dL
|
0.0-1.3 mg/dL
|
|
Direct bilirubin
|
0.4 mg/dL
|
0.0-0.5 mg/dL
|
|
Indirect bilirubin
|
0.9 mg/dL
|
0-1.2 mg/dL
|
|
Serum albumin
|
4.0 g/dL
|
3.5-1.2 g/dL
|
|
Serum globulin
|
2.9 g/dL
|
2.0-3.5 g/dL
|
A differential diagnosis of resolving liver abscess or pancreatic pathology was considered. Further evaluation with 640-slice computed tomography (CT) abdomen showed multiple peripherally enhancing lobulated lesions with internal calcifications involving segments 6, 7 and 8 of right hepatic lobe (Fig. 1 a-f). Few lesions appeared tubular/serpiginous and were located in the subcapsular region (Fig. 2). Imaging was in favor of liver trematodes as the cause of liver abscess. A liver biopsy was done and histopathology of the tissue showed necrotic liver parenchyma with degenerated parts of parasite, likely a trematode (Fig. 3 a and b). Gram stain, acid-fast stain, fungal stain, Xpert Mycobacterium tuberculosis and tissue culture and sensitivity of the sample were negative. Since liver function tests were normal, endoscopic retrograde cholangiopancreatography (ERCP) was deferred and a decision to start medical management was taken. Patient was started on oral nitazoxanide 500 mg 3 times a day for 3 weeks. During follow-up, the patient was found to have no further fever spikes and her right upper quadrant pain had significantly reduced.

Figure 1 (a-f). CT images of liver showing multiple peripherally enhancing lobulated lesions in the right lobe of liver. Few lesions in the subcapsular region can be seen.
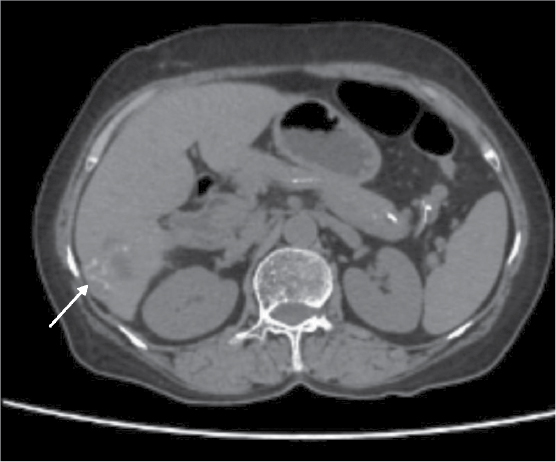
Figure 2. Serpiginous lesion in the subcapsular region.
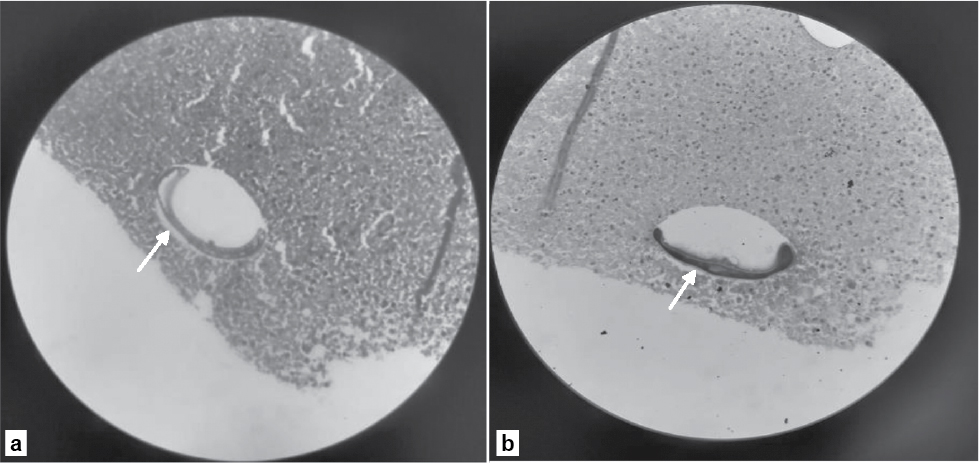
Figure 3 a and b. Histopathology of the liver showing a trematode.
DISCUSSION
Trematodes are unsegmented helminths. They are flat and broad and resemble the leaf of a tree or a flat fish; hence, the name fluke.5 Table 2 describes the comparative analysis of the common liver flukes.6-11
|
Table 2. Comparative Analysis of Common Liver Flukes
|
| |
Opisthorchis
|
C. sinensis
|
Fasciola
|
|
Epidemiology
|
Viverrini: Northeastern Thailand, Laos and Cambodia6
Felineus: Europe and Asia7
|
Asia including Korea, Taiwan, China, Vietnam and Japan8
|
Hepatica: More than 50 countries in all continents except Antarctica
Gigantica: Less widespread
|
|
Definitive host
|
Humans6
|
Humans8
|
Sheep, goats, cattle and humans
|
|
First intermediate host
|
Snail6
|
Snail8
|
Snail
|
|
Second intermediate host
|
Freshwater fish6
|
Freshwater fish8
|
Aquatic plants
|
|
Infective form
|
Metacercariae6
|
Metacercariae8
|
Metacercariae
|
|
Clinical features
|
Viverrini
Acute: Asymptomatic or hepatitis like features6
Chronic: Recurrent cholangitis, cholelithiasis, periductal fibrosis and cholangiocarcinoma6
Felineus
Acute: Fever, abdominal pain, headache, arthralgia, diarrhea, nausea and eosinophilia7
Chronic: Recurrent cholangitis, hepatic abscess, acute pancreatitis and biliary peritonitis7
|
Acute
<100 flukes: Innocuous infection8
>20,000 flukes: Acute cholangitis, jaundice, right upper quadrant pain, nausea, vomiting, anorexia, malaise and fever8
Chronic
Cholelithiasis, pancreatitis, liver abscess and cholangiocarcinoma8
|
Migratory phase (1-4 weeks):
Fever, liver tenderness, urticarial (increased eosinophils) and weight loss9
Complications: Subcapsular hematomas and prolonged febrile illness3
Chronic phase: Cholestatic jaundice, recurrent cholangitis, cholelithiasis, fibrosis of biliary duct9
Complications: Liver abscess, liver fibrosis, cirrhosis, weight loss and anemia9
|
|
Imaging
|
USG: Diffuse to mild intrahepatic biliary duct dilation with intraductal sludge and stones. Sparing of large bile ducts with common bile duct often in normal caliber is seen10
CT: Mild to moderate intrahepatic biliary ductal dilation, predominantly peripheral involvement. Intrahepatic sludge and stones can also be seen10
|
USG: Subcapsular ill-defined hypoechoic mass in parenchymal phase, features of cholangitis in biliary phase10
CT: Capsular thickening, hyperenhancement with peripheral nodular and tortuous lesions corresponding to migratory tract10
|
|
|
Treatment
|
Praziquantel 25 mg/kg in 3 divided doses per day × 2-3 days6
|
Praziquantel 25 mg/kg in 3 divided doses per day × 2-3 days
|
Triclabendazole 2 doses of 10 mg/kg per dose × 12-24 hours
Nitazoxanide 500 mg twice daily × 1 week11
|
Risk factors include travel to endemic areas, consumption of raw or uncooked fish and low socioeconomic status. Most of the patients present with fever, right upper quadrant pain, eosinophilia and anemia.9 As our patient had fever, right upper quadrant pain, loss of appetite, and generalized weakness with serpiginous pattern in CT and liver biopsy showed trematode, a diagnosis of liver abscess due to trematodes was confirmed. Based on the review of existing evidence from several clinical and experimental studies O. viverrini is found to be a definite cause of bile duct carcinoma, while C. sinensis is considered as a probable cause of carcinoma. O. felineus, on the other hand, has not been studied sufficiently.12 Clonorchis and Opisthorchis are associated with recurrent pyogenic cholangitis and pigment stones.13
CONCLUSION
This case report underscores the importance of increasing awareness regarding liver abscess caused by trematodes as a potential differential diagnosis in patients with fever, abdominal pain and eosinophilia. It also highlights the need for high index of suspicion to diagnose this rare entity.
Declaration
Funding: None.
Patient’s Consent: Telephonic consent was obtained from the patient in view of any anonymity.
Conflict of Interest: None.
Ethical Approval: Not required.
REFERENCES
- Akhondi H, Sabih DE. Liver Abscess. [Updated 2023 Jul 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538230/.
- Chai JY, Jung BK. Epidemiology of trematode infections: an update. In: Toledo R, Fried B (Eds.). Digenetic Trematodes. Advances in Experimental Medicine and Biology, Vol. 1154. Springer, Cham. 2019. https://doi.org/10.1007/978-3-030-18616-6_12.
- Peters L, Burkert S, Grüner B. Parasites of the liver – epidemiology, diagnosis and clinical management in the European context. J Hepatol. 2021;75(1):202-18.
- Braseth AL, Elliott DE, Ince MN. Parasitic infections of the gastrointestinal track and liver. Gastroenterol Clin North Am. 2021;50(2):361-81.
- Paniker CKJ, Ghosh S. Paniker’s Textbook of Medical Parasitology. 7th Edition. p.138.
- Liau MYQ, Toh EQ, Shelat VG. Opisthorchis viverrini—current understanding of the neglected hepatobiliary parasite. Pathogens. 2023;12(6):795.
- Pozio E, Armignacco O, Ferri F, Morales MAG. Opisthorchis felineus, an emerging infection in Italy and its implication for the European Union. Acta Trop. 2013;126(1):54-62.
- Locke V, Kusnik A, Richardson MS. Clonorchis Sinensis. [Updated 2022 Dec 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532892/
- Matin S, Joukar F, Yeganeh S, Daryakar A, Mansour-Ghanaei F. Liver abscess due to Fasciola hepatica: a case report of the North of Iran. Case Rep Infect Dis. 2022:2022:4399061.
- Alabousi A, Patlas MN, Khalili K, Haider EA. Parasitic liver infections: imaging findings and strategies for timely diagnosis. Curr Probl Diagn Radiol. 2020;49(6):447-51.
- Ekpanyapong S, Reddy KR. Fungal and parasitic infections of the liver. Gastroenterol Clin North Am. 2020;49(2):379-41.
- Watanapa P, Watanapa WB. Liver fluke-associated cholangiocarcinoma. Br J Surg. 2002;89(8):962-70.
- Chan WW, Showler A, Boggild AK. Parasitic liver disease in travelers. Infect Dis Clin North Am. 2012;26(3):755-80.
|