Published in IJCP
December 2023
Brief Communication
Optimizing Finerenone Therapy: A Comprehensive Review Using the “Finerenone Pentad”
December 11, 2023 | Sourabh Sharma, Sanjay Kalra
Nephrology
Abstract
Chronic kidney disease (CKD) is a pressing global health concern, often intertwined with comorbid conditions such as type 2 diabetes mellitus (T2DM) and cardiovascular complications. Managing CKD in T2DM patients requires a multifaceted approach, and emerging therapeutic options are increasingly essential. Finerenone, a selective nonsteroidal mineralocorticoid receptor antagonist, has shown considerable promise in addressing the intricate cardiorenal needs of these patients. To maximize the effectiveness of this therapy, we propose the approach of “Finerenone Pentad” which can be utilized as a checklist while starting and subsequently monitoring the finerenone therapy. This structured approach offers guidance on patient selection, monitoring and outcome evaluation, ensuring a holistic approach to the care of individuals with T2DM and CKD.
Keywords: Chronic kidney disease, type 2 diabetes, selective nonsteroidal mineralocorticoid receptor antagonist
Chronic kidney disease (CKD), often exacerbated by the presence of type 2 diabetes mellitus (T2DM), represents a challenging medical condition, both for patients and health care providers.1 In the search for therapeutic solutions, finerenone has emerged as a promising option.2-4 This selective nonsteroidal mineralocorticoid receptor antagonist (MRA) addresses the cardiovascular and renal complications frequently encountered in T2DM patients with CKD.2 The concept of “Finerenone Pentad” framework provides a comprehensive strategy for optimizing patient selection, monitoring and outcome assessment, with the ultimate aim of enhancing patient care (Table 1 and Fig. 1).
|
Table 1. The Pentad of Finerenone
|
|
Selection Pentad
|
|
|
|
5 points for inclusion
· T2DM with CKD
· Potassium ≤5 mmol/L
· eGFR ≥25 mL/min/1.73 m2
· UACR ≥30 mg/g
· Men and women ≥18 years
|
5 points for exclusion
· With spironolactone/eplerenone
· Strong CYP3A4 inhibitors
· Pregnancy/Lactation
· Severe hepatic impairment (Child-Pugh C)
· Adrenal insufficiency
|
5 points regardless
· Glucophenotype
· LVH and HF status
· Concomitant therapy for diabetes: SGLT2i/insulin therapy/GLP-1RA
· ASCVD status
· Barophenotype
|
|
Monitoring Pentad
· Serum potassium
· UACR
· eGFR
· Blood pressure
· Serum creatinine
|
Outcome Pentad
· Reduced risk of ESKD by 1/5
· Reduced risk of HHF by >1/5
· Reduced UACR by 32%
· Reduced cardiovascular mortality risk by 12%
· Low clinical impact of hyperkalemia with incidence rate of permanent discontinuation at 1.7%
|
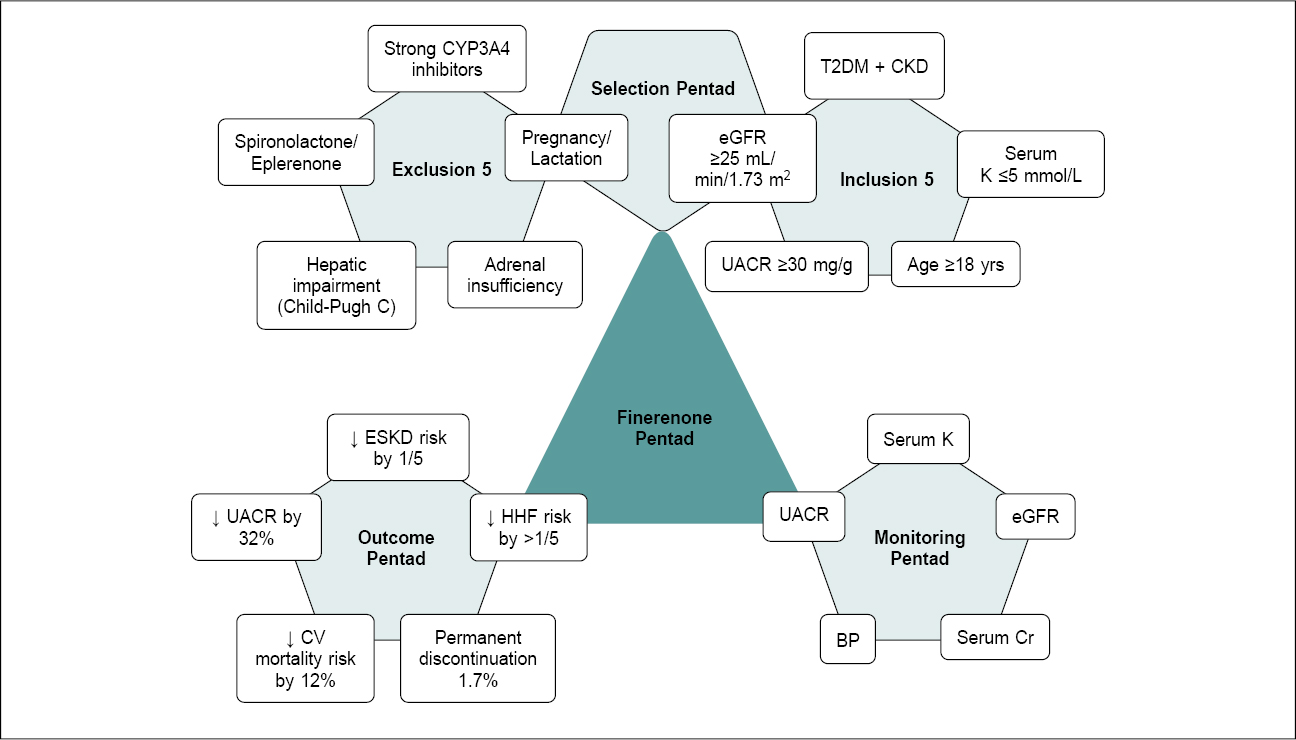
Figure 1. Finerenone Pentad.
THE PATIENT SELECTION PENTAD
In the first component of the “Finerenone Pentad”, the focus is on selecting the most suitable patients for finerenone therapy. To qualify for this treatment, individuals should present a combination of specific inclusion and exclusion criteria.
- Inclusion criteria: These encompass five crucial points, including a diagnosis of T2DM with CKD, potassium levels ≤5 mmol/L, estimated glomerular filtration rate (eGFR) ≥25 mL/min/1.73 m², a urine albumin-to-creatinine ratio (UACR) of ≥30 mg/g and men and women above ≥18 years.2-4 These criteria ensure that the therapy is directed toward patients who stand to benefit the most from finerenone’s cardiorenal protective effects.
- Exclusion criteria: Five specific factors necessitate the exclusion of certain patients. These encompass those already receiving spironolactone or eplerenone, concomitant use with strong CYP3A4 inhibitors, pregnant or lactating patients, those with severe hepatic impairment (Child-Pugh C), and those diagnosed with adrenal insufficiency.2-5 These exclusions help prevent potential complications and ensure patient safety.
- Universal nondiscriminatory criteria: Apart from the defined inclusion and exclusion criteria, there is no requirement for additional considerations when prescribing finerenone. The medication can be administered irrespective of the patient’s glucophenotype (including glycated hemoglobin [HbA1c] levels and T2D duration),6 barophenotype,7 concomitant therapy for diabetes (sodium-glucose cotransporter-2 inhibitor [SGLT2i]/insulin/glucagon-like peptide-1 receptor agonist [GLP-1RA]),6,8,9 atherosclerotic cardiovascular disease (ASCVD),10 left ventricular hypertrophy (LVH) and heart failure (HF) status.11,12
THE MONITORING PENTAD
Upon selecting patients for finerenone therapy, the monitoring phase incorporates consideration of a few specific parameters. The following aspect of the framework delineates five essential factors that health care professionals should observe during the treatment course to assess and monitor the prognostic outcomes of the patients.
- Serum potassium: Due to its distinct structure and mode of action (MoA), the rates and intensity of hyperkalemia is significantly lower compared to steroidal MRA (Spironolactone) as noted in Phase II clinical trials and Amber like post hoc subanalysis.13,14 However, regular monitoring is imperative to mitigate potential adverse events. The proposed potassium monitoring protocol suggests an initial assessment after 1 month of drug initiation to allow for optimal stabilization. Subsequent evaluations, following the standard protocol, are recommended every 4 months if the patient remains stable. In the event of potassium levels going beyond 5.5 mmol/L, it is advised to withhold the drug for a minimum of 72 hours and reintroducing it when levels fall below 5 mmol/L.2-4
- Blood pressure: Hypertension is a common concern in CKD patients. Regular blood pressure monitoring is essential to maintain optimal cardiovascular health, as well as to monitor the control of hypertension.15 Finerenone is noted to cause a mild reduction in blood pressure levels to the tune of 3-4 mmHg in the doses recommended for CKD with T2DM3 as opposed to steroidal MRAs13 and is not a primary therapeutic objective, which hinges primarily on its anti-inflammatory and antifibrotic properties.
- UACR: It offers valuable insights into kidney function and the progression of kidney disease.16 Regular assessments enable health care providers to gauge the effectiveness of finerenone therapy in slowing the deterioration of renal function.
- eGFR: eGFR is a critical parameter for assessing kidney function.16,17 Continuous monitoring helps clinicians make necessary adjustments to therapy and ensures that the treatment aligns with the patient’s renal status.
- Serum creatinine: Regular assessments of serum creatinine levels provide crucial information about kidney function and the impact of therapy.18 This parameter aids health care professionals in gauging the patient’s renal health over time.
eGFR and serum creatinine are important parameters for assessment of renal function alongside UACR.16-18 The use of finerenone demonstrates a potential reduction in the decline of eGFR within 12 months. However, a mild initial eGFR decline of 3-4 mL may occur in the first 1-4 months of finerenone initiation, this typically remains within 30% mirroring the pattern seen with many renal protective drugs. There have been no increased incidences of acute kidney injury noted with finerenone in the Phase III clinical trials.2,4
The transient decline in GFR noted with many renoprotective drugs such as angiotensin-converting enzyme inhibitors (ACEIs)/angiotensin receptor blockers (ARBs) or SGLT2i is a pharmacological effect leading to a new physiological renal function set point.19
Patient education plays a really crucial role here so as to prevent undue alarm, as this initial dip aligns with the drug’s long-term renal stabilization effect.
THE OUTCOME PENTAD
The final component of the “Finerenone Pentad” outlines specific outcomes that therapy aims to achieve or evaluate during the treatment process. These outcomes are quintessential in assessing the success of finerenone therapy.
- Reduced risk of ESKD: A primary objective of finerenone therapy is to slow down the progression of kidney disease and subsequently the risk of end-stage kidney disease (ESKD), which has been seen to be reduced by 20%.2,3 ESKD poses significant challenges for patients and is often associated with a reduced quality of life.20 The reduction in ESKD risk represents a major benefit for individuals receiving this treatment.
- Reduced risk of HHF: Hospitalization for heart failure (HHF) is a critical concern in patients with T2DM and CKD.21 Therapy aims to reduce the risk of HHF by more than 20%,2,3 further improving the patient’s quality of life and reducing the burden on health care resources.
- Reduced UACR: Another key outcome is the reduction in UACR by 32%,3 and this change is seen within 1-4 months of initiation with finerenone and is sustained. This decrease signifies an improvement in kidney function and a slowing of kidney disease progression as well as provides significant cardiovascular risk benefit.
- Reduced cardiovascular mortality: In addition to renal benefits, finerenone therapy aims to lower cardiovascular mortality risk by 12%22 and sudden cardiac death by 25%.22 Cardiovascular events are a major cause of morbidity and mortality in this patient population,23 and this reduction represents a significant improvement in overall patient outcomes.
- Low clinical impact of hyperkalemia: Managing hyperkalemia is a common concern with MRAs.2 Despite a hyperkalemia incidence rate of 14% compared to placebo in FIDELITY analysis, clinical impact rates were minimal, with a specific incidence rate of permanent discontinuation set at 1.7%.3 With an average increase of 0.2 mmol, only 4.5% of the patients exceeded a potassium level of 6 mmol/L.24 This ensures the safety and tolerability of the treatment.
RECOMMENDED POSITIONING OF FINERENONE FOR CARDIORENAL PROTECTION
Over the past few years, there has been a notable paradigm shift in the management of patients, from an organ-specific strategy to a more holistic patient-centric approach, with guidelines recommending regular routine screening of individuals with T2D using UACR and eGFR for early diagnosis of CKD and cardiovascular risk, along with a multifactorial approach towards management. In addition to the traditional standard of care including lifestyle modifications, glycemic control, blood pressure regulation and lipid management, which form the cornerstone/foundation of therapy, agents conferring cardiovascular and kidney benefits such as ACEIs/ARBs, SGLT2i and finerenone have firmly established themselves as the “three pillars” of therapy for slowing kidney disease progression and reducing development of heart failure and risk of cardiovascular death in patients with CKD in T2D, with a Level A recommendation for these drugs.25-28 Nonsteroidal MRAs like finerenone are now recommended along with other medications for cardiovascular and kidney protection rather than as alternatives when other treatments have not been effective.26
A proposed approach recommends optimizing the dose of ACEI/ARB to a maximally tolerated level initially and subsequently introducing the other two drugs, i.e., Finerenone and SGLT2i with at least a week’s interval in between to allow for equilibration of kidney function before the addition of the next agent.28 Early initiation of combination therapy with this triad is advocated due to their distinct yet complementary MoA facilitating a more comprehensive disease management approach.29
CONCLUSIONS
The “Finerenone Pentad” is a comprehensive, patient-centric framework that empowers health care professionals to provide high-quality care for individuals with T2DM and CKD. By following the selection, monitoring and outcome criteria, clinicians can offer a well-rounded approach to address the complex cardiorenal needs of these patients.
In conclusion, this framework allows for the effective optimization of finerenone therapy. The structured approach empowers health care providers to make data-driven decisions, targeting the reduction of ESKD, HHF, cardiovascular mortality and other complications while ensuring the safe and effective management of hyperkalemia.
Author Contributions
All authors contributed substantially to the article concept and were accountable for the accuracy of the information contained in the article.
Acknowledgment
The authors wish to acknowledge Dr Pravin Manjrekar, Dr Amaninder Mann and Dr Aparajita Praharaj for data support and review of the manuscript.
Data Availability
No datasets were used in the development of this manuscript.
Financial Support and Sponsorship
Nil. Bayer did not support via grant or payment the development of this publication.
Competing Interests
Pravin Manjrekar, Aparajita Praharaj and Amaninder Mann are employees of Bayer.
REFERENCES
- Thomas MC, Cooper ME, Zimmet P. Changing epidemiology of type 2 diabetes mellitus and associated chronic kidney disease. Nat Rev Nephrol. 2016;12(2):73-81.
- Bakris GL, Agarwal R, Anker SD, Pitt B, Ruilope LM, Rossing P, et al; FIDELIO-DKD Investigators. Effect of finerenone on chronic kidney disease outcomes in type 2 diabetes. N Engl J Med. 2020;383(23):2219-29.
- Agarwal R, Filippatos G, Pitt B, Anker SD, Rossing P, Joseph A, et al; FIDELIO-DKD and FIGARO-DKD investigators. Cardiovascular and kidney outcomes with finerenone in patients with type 2 diabetes and chronic kidney disease: the FIDELITY pooled analysis. Eur Heart J. 2022;43(6):474-84.
- Filippatos G, Anker SD, Agarwal R, Ruilope LM, Rossing P, Bakris GL, et al; FIGARO-DKD Investigators. Finerenone reduces risk of incident heart failure in patients with chronic kidney disease and type 2 diabetes: analyses from the FIGARO-DKD trial. Circulation. 2022;145(6):437-47.
- Heinig R, Lambelet M, Nagelschmitz J, Alatrach A, Halabi A. Pharmacokinetics of the novel nonsteroidal mineralocorticoid receptor antagonist finerenone (BAY 94-8862) in individuals with mild or moderate hepatic Eur J Drug Metab Pharmacokinet. 2019;44(5):619-28.
- McGill JB, Agarwal R, Anker SD, Bakris GL, Filippatos G, Pitt B, et al; FIDELIO-DKD and FIGARO-DKD investigators. Effects of finerenone in people with chronic kidney disease and type 2 diabetes are independent of HbA1c at baseline, HbA1c variability, diabetes duration and insulin use at baseline. Diabetes Obes Metab. 2023;25(6):1512-22.
- Ruilope LM, Agarwal R, Anker SD, Filippatos G, Pitt B, Rossing P, et al; FIDELIO-DKD Investigators. Blood pressure and cardiorenal outcomes with finerenone in chronic kidney disease in type 2 diabetes. Hypertension. 2022;79(12):2685-95.
- Rossing P, Agarwal R, Anker SD, Filippatos G, Pitt B, Ruilope LM, et al; FIDELIO-DKD Investigators. Efficacy and safety of finerenone in patients with chronic kidney disease and type 2 diabetes by GLP-1RA treatment: a subgroup analysis from the FIDELIO-DKD trial. Diabetes Obes Metab. 2022;24(1):125-34.
- Rossing P, Anker SD, Filippatos G, Pitt B, Ruilope LM, Birkenfeld AL, et al; FIDELIO-DKD and FIGARO-DKD Investigators. Finerenone in patients with chronic kidney disease and type 2 diabetes by sodium-glucose cotransporter 2 inhibitor treatment: the FIDELITY analysis. Diabetes Care. 2022;45(12):2991-8.
- Filippatos G, Anker SD, Pitt B, McGuire DK, Rossing P, Ruilope LM, et al. Finerenone efficacy in patients with chronic kidney disease, type 2 diabetes and atherosclerotic cardiovascular disease. Eur Heart J Cardiovasc Pharmacother. 2022;9(1):85-93.
- Matavelli L, Filippatos G, Anker SD, Bakris GL, Rossing P, Ruilope LM, et al. Finerenone in chronic kidney disease and type 2 diabetes: a FIDELITY analysis of left ventricular hypertrophy. Am J Prev Cardiol. 2023;15:100544.
- Filippatos G, Pitt B, Agarwal R, Farmakis D, Ruilope LM, Rossing P, et al; FIDELIO-DKD Investigators. Finerenone in patients with chronic kidney disease and type 2 diabetes with and without heart failure: a prespecified subgroup analysis of the FIDELIO-DKD trial. Eur J Heart Fail. 2022;24(6):996-1005.
- Kintscher U, Bakris GL, Kolkhof P. Novel non-steroidal mineralocorticoid receptor antagonists in cardiorenal disease. Br J Pharmacol. 2022;179(13):3220-34.
- Agarwal R, Pitt B, Palmer BF, Kovesdy CP, Burgess E, Filippatos G, et al. A comparative post hoc analysis of finerenone and spironolactone in resistant hypertension in moderate-to-advanced chronic kidney disease. Clin Kidney J. 2022;16(2):293-302.
- Carey RM, Muntner P, Bosworth HB, Whelton PK. Prevention and Control of Hypertension: JACC Health Promotion Series. J Am Coll Cardiol. 2018;72(11):1278-93.
- Lopez-Giacoman S, Madero M. Biomarkers in chronic kidney disease, from kidney function to kidney damage. World J Nephrol. 2015;4(1):57-73.
- Zsom L, Zsom M, Salim SA, Fülöp T. Estimated glomerular filtration rate in chronic kidney disease: a critical review of estimate-based predictions of individual outcomes in kidney disease. Toxins (Basel). 2022;14(2):127.
- Levey AS, Perrone RD, Madias NE. Serum creatinine and renal function. Annu Rev Med. 1988;39:465-90.
- Bakris GL, Weir MR. Initial drops in glomerular filtration rate with certain drug classes retard kidney disease progression. Am J Nephrol. 2022;53(7):513-5.
- Chen SS, Al Mawed S, Unruh M. Health-related quality of life in end-stage renal disease patients: how often should we ask and what do we do with the answer? Blood Purif. 2016;41(1-3):218-24.
- Vijay K, Neuen BL, Lerma EV. Heart failure in patients with diabetes and chronic kidney disease: challenges and opportunities. Cardiorenal Med. 2022;12(1):1-10.
- Filippatos G, Anker SD, August P, Coats AJS, Januzzi JL, Mankovsky B, et al. Finerenone and effects on mortality in chronic kidney disease and type 2 diabetes: a FIDELITY analysis. Eur Heart J Cardiovasc Pharmacother. 2023;9(2):183-91.
- Ardhanari S, Alpert MA, Aggarwal K. Cardiovascular disease in chronic kidney disease: risk factors, pathogenesis, and prevention. Adv Perit Dial. 2014;30:40-53.
- Agarwal R, Joseph A, Anker SD, Filippatos G, Rossing P, Ruilope LM, et al; FIDELIO-DKD Investigators. Hyperkalemia risk with finerenone: results from the FIDELIO-DKD trial. J Am Soc Nephrol. 2022;33(1):225-37.
- Kidney Disease: Improving Global Outcomes (KDIGO) Diabetes Work Group. KDIGO 2022 Clinical Practice Guideline for Diabetes Management in Chronic Kidney Disease. Kidney Int. 2022;102(5S):S1-S127.
- ElSayed NA, Aleppo G, Aroda VR, Bannuru RR, Brown FM, Bruemmer D, et al, on behalf of the American Diabetes Association. 11. Chronic Kidney Disease and Risk Management: Standards of Care in Diabetes-2023. Diabetes Care. 2023;46(Suppl 1):S191-S202.
- de Boer IH, Khunti K, Sadusky T, Tuttle KR, Neumiller JJ, Rhee CM, et al. Diabetes management in chronic kidney disease: a consensus report by the American Diabetes Association (ADA) and Kidney Disease: Improving Global Outcomes (KDIGO). Diabetes Care. 2022;45(12):3075-90.
- Blazek O, Bakris GL. The evolution of “pillars of therapy” to reduce heart failure risk and slow diabetic kidney disease progression. Am Heart J Plus: Cardiol Res Pract. 2022;19:100187.
- Fioretto P, Pontremoli R. Expanding the therapy options for diabetic kidney disease. Nat Rev Nephrol. 2022;18(2):78-79.
|