Published in IJCP
January 2024
Consensus statement
Consensus on Stroke Prevention in Atrial Fibrillation and Utilization of NOACs in the Real-World Setting in India
January 11, 2024 | Ponde CK, Shah VT, Shah Dhiren, Khan Aziz, Verma Gaurav, Kochhar Arun, Mahonan PP, Dave Tarun, Dwivedi Shailendra, Narayana Murthy, John Satish, Routray SN, Hazra PK, Bhadury Spandan, Kuladhipati Indra, Sharma AD, Mayabhate MM, Pawar DB
Cardiology
https://doi.org/10.59793/ijcp.v34i8.758
Abstract
Atrial fibrillation (AF) is the most frequent cardiac arrhythmia. Prevention of stroke and systemic thromboembolism remains the cornerstone of the management of AF. Even today, there are unresolved knowledge gaps in AF pathophysiology, screening and therapeutic strategies and stroke prevention. The modified DELPHI method was used to develop the best practice recommendations for the management of AF in a real-world setting with the participation of 500 cardiologists across India. The experts concurred that the decision to initiate antithrombotic treatment in patients with transient AF could be based on the duration of transient AF, the co-existence of the risk factor for stroke and echocardiographic abnormalities impact the decision. The decision to initiate anticoagulant therapy in device-detected atrial high-rate episodes (AHRE) can be decided based on the duration of AHRE, the burden of AHRE and the individual’s risk of stroke and thromboembolism. The benefit of early anticoagulation should be balanced with the risk of intracerebral hemorrhage (ICH), especially in elderly patients and in severe strokes. Apixaban is the preferred drug in patients with concomitant ischemic heart disease (IHD), patients with a history of gastrointestinal (GI) bleeding, patients with underlying malignancy, elderly patients with AF, patients with comorbid diseases and patients with hepatic disease or renal disease. Apixaban was considered to be an affordable novel oral anticoagulant (NOAC) for Indian patients for primary and secondary stroke prophylaxis in AF patients.
Keywords: NOACs, stroke prevention, atrial fibrillation, apixaban, dabigatran
Atrial fibrillation (AF) is the most frequent cardiac arrhythmia affecting 43 million people globally.1 Its incidence and prevalence have increased over the last 20 years and will continue to increase over the next 30 years, especially in countries with a middle socio-demographic index.1 The current European guidelines recommend a holistic AF Better Care (ABC) pathway, involving anticoagulation to avoid stroke, improved control of symptoms and approaches for the reduction of cardiovascular events.
Despite significant advances in its detection, mechanistic understanding and management, AF continues to have a major impact on the morbidity and mortality of millions of patients, partly because of unresolved knowledge gaps in its pathophysiology, screening and therapeutic strategies and stroke prevention. The development of actionable personalized approaches, which take into account patient-specific profiles will be essential to overcome the current challenges in AF management.2
Prevention of stroke and systemic thromboembolism remains the cornerstone for the management of AF.3 Despite the strong association with stroke, there is no evidence that screening for AF in asymptomatic patients improves clinical outcomes. The clinical dilemma is identification of patients who should be screened for risk of stroke.4 Similar dilemmas need to be identified and the best possible clinical approach to resolve these dilemmas needs to be developed.
The association between AF and stroke is firmly established, and anticoagulation reduces stroke risk in patients with AF.5 However, the role of anticoagulation is still evolving and many questions about the appropriate use of novel oral anticoagulants (NOACs) for stroke prevention remain to be answered. In the absence of well-designed clinical trials to answer some of these questions, a consensus meeting of Indian cardiologists was convened. Data collection began in July 2022 with the first meeting of 12 key opinion leaders (KOLs) in Mumbai, Maharashtra. The second meeting was conducted at 48 locations across the country in August 2022 with 500 cardiologists.
METHODOLOGY
The modified DELPHI method was used to develop the best practice recommendations for the management of AF in a real-world setting. The DELPHI method has defined the methodology to develop consensus recommendations by enlisting the participation of experts from India. The methodology was conducted in two rounds.
In the first round, the questionnaire was framed by the core group after a literature review. The literature review was done using PubMed database. In Round 2, the questionnaire was administered to 500 cardiologists across India. Voting for answers to the questions was conducted and >70% of votes in favor of the answer were taken as a positive point to frame the consensus statement.
The consensus statements were framed and perused by experts and participants prior to the preparation of the manuscript for publication (Fig. 1).
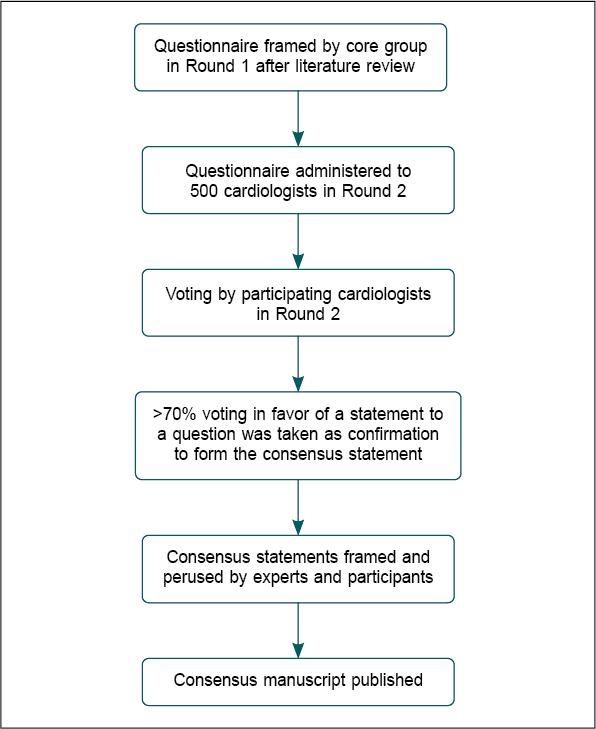
Figure 1. The DELPHI methodology followed for framing the consensus statements.
Which are the Populations Ideal for Screening of AF in a Real-World Setting?
Background
A wide range of risk factors have been identified for AF including coronary heart disease, hypertension (>140/90 mmHg), heart failure (HF) (with reserved and preserved ejection fraction), chronic obstructive pulmonary disease, left ventricular diastolic dysfunction, diabetes, hyperthyroidism, obesity, left atrial dilatation, left ventricular hypertrophy, obstructive sleep apnea (OSA) syndrome, atrial conduction delay/PR interval and chronic kidney disease.6 The core group identified some of these risk factors as commonly seen in their patients in the real-world setting in India.
Patients with mitral stenosis often have AF due to pathogenic events such as left atrial enlargement because of constant pressure and volume overload.7 Both HF and myocardial infarction (MI) are associated with an increased risk of AF and vice versa creating a feed-forward loop that increases mortality.8 OSA is present in 21% to 74% of patients with AF. A structural remodeling as well as transient and acute apnea-associated transient atrial electrophysiological changes can occur as a result of long-term OSA.9 The link between AF and ischemic stroke is strong. The subtype most commonly associated with AF is cardioembolic stroke, which is particularly severe and shows the highest rates of mortality and permanent disability.10 AF increases the risk of stroke fivefolds.11 About 25% to 30% of patients with an ischemic stroke and >80% of those with cardioembolic ischemic stroke have AF.12 A Congestive Heart Failure, Hypertension, Age, Diabetes Mellitus, Prior Stroke or TIA or Thromboembolism, Vascular Disease, Age, Sex Category (CHA2DS2-VASc) score ≥3 has been associated with about 3.2 stroke events per year.11 Patients with coronary artery disease (CAD) and a dual or triple chamber implantable cardioverter-defibrillator (ICD) show a high incidence of device-detected AF.13 The prevalence of AF increases exponentially with age. It is reported to be about 9.9% at age 70 to 79 and 23.5% at age 80 to 89.14 Two-thirds of patients with AF are aged over 75 years.15
Recommendations from guidelines
The 2020 European Society of Cardiology (ESC) guidelines for AF recommend opportunistic screening for AF in hypertensive patients as well as in patients with OSA.16
Experts’ polling responses
The analysis of the DELPHI voting is presented in Table 1.
|
Table 1. The DELPHI Voting Analysis
|
|
Criteria
|
Voting in favor (%)
|
|
Mitral stenosis
|
71
|
|
Echocardiogram with unexplained left atrial enlargement
|
89
|
|
Patients with ≥2 vascular risk factors (CHA2DS2-VASc score ≥3)
|
90
|
|
Patients with sleep apnea
|
83
|
|
Obese patients
|
76
|
|
Intracardiac device patients
|
76
|
|
Stroke patients (cryptogenic and ischemic)
|
90
|
|
All persons >75 years of age
|
84
|
|
Consensus statement 1
The populations ideal for screening of AF in a real-world setting include obese patients, intracardiac device patients, stroke patients (cryptogenic and ischemic), patients with mitral stenosis, unexplained left atrial enlargement on echocardiogram, sleep apnea, patients with ≥2 vascular risk factors (CHA2DS2-VASc score ≥3) and all persons >75 years of age.
|
What should be the Approach to Decide Whether Antithrombotic Therapy is Required for the Management of Transient AF?
Background
Currently, AF is usually diagnosed based on intermittent electrocardiogram (ECG) or external event monitors. But with this approach, one may miss the diagnosis of paroxysmal AF in an outpatient until complications such as systemic embolization ensue. Secondly, patients may be over-treated with oral anticoagulants (OACs), when in fact it may not be warranted, based on the AF burden and significant bleeding risk as defined by HAS-BLED (Hypertension, Abnormal Renal/Liver Function, Stroke, Bleeding History or Predisposition, Labile International Normalized Ratio [INR], Elderly [age ≥65 years], Drugs/Alcohol Concomitantly) score ≥3.
Often, a patient may not be in AF chronically, and the AF burden (the amount of time the patient is in AF out of the total monitored time) is not calculated. An AF burden of ≥1 hour daily is postulated to be associated with a higher risk of embolization. In patients with a history of AF who maintain normal sinus rhythm or in patients with low AF burden, long-term OACs may be more harmful than beneficial. This is especially true in the elderly population with high risk of bleeding.17 Hence, it is critical to identify the clinical context and carefully consider the risk-benefit ratio of all approaches when making treatment decisions.17
The association between AF and stroke is well known, and the use of anticoagulants lowers the risk of stroke in patients with AF.5
Currently, data is awaited regarding the minimal amount of subclinical AF, which validates the use of anticoagulants for stroke prevention.5
Recommendations from guidelines
- Anatomical imaging provides the left atrium (LA) size, shape and fibrosis. The most accurate assessment of LA dilation is obtained by cardiac magnetic resonance (CMR) or computed tomography (CT). For routine assessment, two-dimensional (2D) or (preferably) three-dimensional (3D) transthoracic echocardiography is used. The 3D echocardiographic normal volume values are 15-42 mL/m2 for men and 15-39 mL/m2 for women.
- In patients with AF initially at low risk of stroke, the first reassessment of stroke risk should be made 4 to 6 months after the index evaluation.18
- In AF patients with stroke risk factors not taking OAC before ablation, it is recommended that pre-procedural management of stroke risk includes initiation of anticoagulation and preferably, therapeutic OAC for at least 3 weeks before ablation or alternatively, the use of transesophageal echocardiography (TEE) to exclude LA thrombus before ablation.18
Experts’ polling responses
The experts concurred that the decision to initiate antithrombotic treatment in patients with transient AF could be based on the duration of transient AF; the co-existence of the risk factor for stroke and echocardiographic abnormalities also impact the decision (Table 2).
|
Table 2. Factors Affecting Antithrombotic Drug Initiation in Patients with Transient AF
|
|
Criteria
|
Voting in favor (%)
|
|
Duration of transient AF
|
80
|
|
Co-existence of the risk factor for stroke
|
93
|
|
Echocardiographic abnormalities
|
91
|
|
Consensus statement 2
The decision whether antithrombotic management of transient AF is indicated can be decided based on the duration of transient AF, the co-existence of the risk factor for stroke and echocardiographic abnormalities.
|
What are the Factors Affecting the Initiation of Anticoagulation Therapy in Patients with Device-detected AHRE?
Background
Cardiac implanted electronic devices (CIEDs) help in the detection of self-terminating atrial arrhythmias commonly, e.g., atrial high-rate episodes (AHREs), which are also termed subclinical atrial tachyarrhythmia or subclinical AF. The reported incidence of AHRE varies considerably from 10% to 70%.19 Patients with device-detected AHREs are at an elevated risk of stroke and may have unmet anticoagulation needs.20AHRE episodes ≥5 minutes are associated with a higher risk of ischemic stroke. The absence of randomized trials to explore the place of anticoagulation therapy in patients with device-detected AHRE makes the management of these patients challenging studies. Currently, treatment with anticoagulants like NOACs must be individualized.21 Based on current data, antithrombotic therapy can be advocated in patients without documented AF showing AHRE >24 hours and a CHA2DS2-VASc score ≥1.22 The European Heart Rhythm Association (EHRA) recommends anticoagulation for patients with AHRE ≥5.5 hours per day and a CHA2DS2-VASc score of ≥2 (≥3 in females). Anticoagulation could be recommended for CHA2DS2-VASc scores of 1 (2 in females). In patients with several risk factors, anticoagulation should be considered even in cases with a shorter duration of AHRE.23 In HF patients, device-detected atrial arrhythmias are associated with an increased incidence of thromboembolic events. A cut-off point of 3.8 hours over 24 hours has been observed to be associated with significant increase in the event rate. Anticoagulation initiation and the optimization of cardioprotective HF therapy could be useful in this patient population.24
Recommendations from guidelines
Structured characterization of AF, which includes clinical assessment of stroke risk, symptom status, burden of AF and evaluation of substrate, should be considered in all AF patients, to streamline the assessment of AF patients at different health care levels, inform treatment decision-making and facilitate optimal management of AF patients (IIa).25
Experts’ polling responses
The duration of AHRE and the burden of AHRE were the two factors that were voted for by the experts (Table 3).
|
Table 3. Application of Anticoagulation Therapy in Patients with Device-detected AHRE
|
|
Criteria
|
Voting in favor (%)
|
|
Duration of AHRE
|
86
|
|
The burden of AHRE
|
87
|
|
The individual’s risk of stroke and thromboembolism
|
92
|
|
Consensus statement 3
The decision to initiate anticoagulant therapy in patients with device-detected AHRE can be decided based on the duration of AHRE, the burden of AHRE, and the individual’s risk of stroke and thromboembolism.
|
What is the Optimal Timing of Initiating Anticoagulation Therapy with NOACs in Elderly Patients with Valvular AF and Ischemic Stroke?
Background
The prevalence of AF increases with age, ranging from approximately 9% to 17% in adults aged 80 years.26 Elderly patients have a challenging set of clinical issues such as a decline in renal function, altered body composition and a high risk of falling. The bleeding risk associated with warfarin in the elderly is a much-debated issue. The benefit-risk ratio must be considered when choosing the strategies for antithrombotic therapies in this population.27 The elderly population, especially those ≥75 years, is often underrepresented in clinical trials. But, almost 40% of the trial population in large NOAC approval studies consists of the elderly.28
Primary and secondary prevention of stroke in elderly patients poses a challenge due to the escalation of both thrombotic and hemorrhagic risks with age. Hence, there is often a delay in the initiation of NOACs in the elderly population after an AF-related ischemic stroke, a stroke of the undetermined cause, after intracranial bleeding or in a high-risk bleeding situation associated with stroke in the real-world setting.29
With the advent of new NOACs such as apixaban, early anticoagulation in the elderly population has become a strategy for stroke prevention. The Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) study included the elderly population (39% aged 65-74 years, 18% aged 75-79 years and 13% aged ≥80 years).26 Apixaban was associated with less major bleeding, less total bleeding and less intracranial hemorrhage regardless of age. The absolute benefits of apixaban were greater in the older population.30 Data from phase III clinical trials on AF indicate that apixaban and edoxaban in elderly patients were associated with the highest reduction of extracranial bleeding events versus warfarin.26 All patients ≥75 years of age are recommended to receive OAC with a Class Ia recommendation irrespective of the presence or absence of additional risk factors.31,32
Recommendations from guidelines
Though infarct size/stroke severity is used clinically to guide the timing of OAC initiation, the usefulness of such an approach in estimating the net benefit of early treatment may be limited. Strong evidence to comment on the optimal timing for (re)initiation of OAC after acute stroke is currently not available. From the cardiological perspective, OAC should be (re)initiated as soon as considered possible from the neurological perspective (in most cases within the first 2 weeks).
In AF patients, who presented with acute ischemic stroke despite taking OAC, optimization of OAC therapy is of key importance—if on vitamin K antagonist (VKA), optimize time in therapeutic range (TTR) (ideally >70%) or switch to a NOAC; if on NOAC, ensure appropriate dosing and good adherence to treatment. Inappropriate NOAC under-dosing using lower or reduced doses of specific NOACs has been associated with an increased risk of stroke/systemic embolism, hospitalization and deaths without appreciable reduction in major bleeding.18
Experts’ polling responses
The experts opined that the benefit of early anticoagulation should be balanced with the risk of intracerebral hemorrhage (ICH), especially in elderly patients and in severe strokes. The age of the patients does affect the decision about the best time to initiate anticoagulant treatment; however, this criterion did not meet the predetermined cut-off value of >70% to merit inclusion in the consensus statement (Table 4).
|
Table 4. Factors Affecting Optimal Timing of Initiating Anticoagulation Therapy
|
|
Criteria
|
Voting in favor (%)
|
|
The benefit of early anticoagulation should be balanced with the risk of ICH, especially in elderly patients and in severe strokes.
|
94
|
|
The decision of timing will be affected by the patient’s age.
|
69
|
|
Consensus statement 4
The benefit of early anticoagulation should be balanced with the risk of ICH, especially in elderly patients and in severe strokes.
|
Which Parameters Must be Considered When Choosing the Most Appropriate NOAC in Order of Significance?
Background
There are scant trials conducting a head-to-head comparison of different NOACs to ascertain the choice of a NOAC in diverse patient populations.33 The factors affecting the choice of a NOAC include age, gender, comorbid conditions, bleeding risk, CHA2DS2-VASc and HAS-BLED scores, concomitant medications, hypertension, history of bleeding, alcohol abuse, renal function and hepatic function.34
A retrospective registry-based cohort study (n = >50,000 patients of AF) by Gundlund et al evaluated patients treated with a NOAC (dabigatran, rivaroxaban or apixaban) using the comprehensive Danish health databases. A subanalysis demonstrated that patients with a prior intracranial hemorrhage were more likely to be initiated on apixaban compared with a VKA (OR 1.42, 95% confidence interval [CI] 1.09-1.86). Further, patients who had previously suffered from gastrointestinal (GI) bleeding were less likely to be initiated on rivaroxaban compared with a VKA (OR 0.84, 95% CI 0.73-0.97). Patients treated with dabigatran were younger and had lower CHA2DS2-VASc and HAS-BLED scores, whereas patients treated with either rivaroxaban or apixaban were generally older than those initiated on VKAs. Additionally, patients initiated on apixaban had higher predicted risk scores than those initiated on VKAs.31,35
In elderly population, the higher risk of bleeding has to be considered when making the choice of NOAC. The Randomized Evaluation of Long-term Anticoagulant Therapy (RE-LY) trial showed that in patients with AF (aged ≥75 years), a lower dabigatran dose (110 mg twice daily) was observed to be associated with major bleeding rates comparable to warfarin. A higher dose (150 mg twice daily), however, resulted in a higher risk of major bleeding. This prompted the recommendation to use only a lower dabigatran dose (110 mg twice daily) in patients older than 80 years.36 The ARISTOTLE study included 39% of patients who were aged 65 to 74 years, 18% 75 to 79 years and 13% >80 years. In this study, apixaban treatment resulted in decreased major bleeding, total bleeding and intracranial hemorrhage than the comparator treatment, warfarin, regardless of age.30
Park et al conducted a cross-sectional analysis of NOAC-using patients with nonvalvular AF (NVAF) (n = 6,061 patients) who were aged ≥65 years on the index date. Patients aged ≥75 years and women were more likely to use apixaban relative to rivaroxaban. Patients with prior stroke/transient ischemic attack (TIA)/thromboembolism had higher odds of using dabigatran and apixaban. Patients with renal disease had increased odds of using apixaban. These findings are consistent with the efficacy and safety profiles reported in pivotal trials and observational studies comparing individual NOACs.37
The factors influencing OAC prescription for AF are not well understood. Hence, the current DELPHI method was adopted to understand the factors affecting the choice of NOAC by Indian experts in the real-world setting based on their experience with different NOACs.
Recommendations from guidelines
- For bleeding risk assessment, a formally structured risk-score-based bleeding risk assessment is recommended to help identify nonmodifiable and address modifiable bleeding risk factors in all AF patients and to identify patients potentially at high risk of bleeding who should be scheduled for early and more frequent clinical review and follow-up. Bleeding risk scores should be considered in AF patients on OAC to identify modifiable risk factors for major bleeding.
- For patients undergoing AF catheter ablation who have been therapeutically anticoagulated with warfarin, dabigatran, rivaroxaban, apixaban or edoxaban, the performance of the ablation procedure without OAC interruption is recommended.16
- In patients on VKAs with low time in international normalized ratio (INR) therapeutic range (e.g., TTR <70%)
- Switching to a NOAC but ensuring good adherence and persistence with therapy; or
- Efforts to improve TTR (e.g., education/counseling and more frequent INR checks) (IIA) is recommended.18
Experts’ polling responses
There was no clear consensus regarding the choice of NOAC in diverse patient profiles. But, age, risk of stroke, bleeding risk, comorbidities and renal and hepatic impairment were regarded as important factors to be considered when choosing a NOAC for the patient (Table 5).
|
Table 5. Parameters to Consider When Choosing the NOAC
|
|
Parameters when choosing the most appropriate NOAC
|
Preference (%)
|
|
1st
|
2nd
|
3rd
|
4th
|
5th
|
6th
|
|
Age
|
34
|
12
|
14
|
15
|
13
|
11
|
|
Risk of stroke
|
31
|
23
|
11
|
13
|
14
|
7
|
|
Risk of bleeding
|
31
|
19
|
22
|
13
|
8
|
6
|
|
Comorbidities
|
16
|
15
|
14
|
23
|
25
|
6
|
|
Body weight
|
11
|
10
|
7
|
10
|
27
|
35
|
|
Renal and hepatic impairment
|
25
|
18
|
11
|
14
|
16
|
16
|
|
Consensus statement 5
Apixaban could be the preferred drug in patients with concomitant ischemic heart disease (IHD), patients with a history of GI bleeding and patients with underlying malignancy. Apixaban is the NOAC of choice in the elderly, patients at high risk of stroke, patients at high risk of bleeding, patients with comorbid diseases and patients with hepatic disease or renal disease. Apixaban can be considered to be an affordable NOAC in India.
|
Which Oral Anticoagulant should be Chosen for Stroke Prevention in AF?
Background
It is a difficult task to choose the best OAC for stroke prevention, as the treating physician must be vigilant that the drug being used provides a complete protection from future thromboembolic conditions, while at the same time does not pose a threat for bleeding disorders. As the search continues, it is all the more important to consider the comorbid conditions in the patients like hepatic and renal impairment, advancing age, the use of multiple drugs, pre-existing bleeding conditions, etc. before choosing the therapy. Thus, the best OAC drug for each patient has to be individualized as per the personal medical history and comorbidities.38
Recommendations from guidelines
All 4 pivotal clinical trials comparing individual direct oral anticoagulants (DOACs) like apixaban, dabigatran, edoxaban and rivaroxaban with warfarin showed superiority or noninferiority to warfarin for the prevention of stroke or systemic embolism in patients with AF except for moderate to severe mitral stenosis or mechanical heart valve. GI bleeding risks were significantly higher in the dabigatran 150 mg twice daily, edoxaban 60 mg once daily and rivaroxaban groups compared with the warfarin group. However, the apixaban group did not significantly increase the risk of GI bleeding compared with the warfarin group. Similarly, edoxaban and dabigatran are contraindicated in patients with creatinine clearance (CrCl) <15 mL/hour or on dialysis, while apixaban and rivaroxaban can be used in such population. Hence, multiple factors need to be considered before choosing the most suitable OAC.38
Experts’ polling responses
A poll was sought to seek the opinion of the cardiologists in the meetings about their preference for apixaban in diverse patient profiles. In patients at high risk of bleeding, patients with a previous history of GI bleed and patients with renal disease, apixaban was preferred by >80% of the respondents over the other NOACs. Their opinions were based on the evaluation of the efficacy and safety reports of apixaban and also on their experience with apixaban in a real-world setting in India (Table 6).
|
Table 6. Voting in Favor of Apixaban as 1st Choice
|
|
Patient conditions
|
Voting in favor of apixaban as 1st choice (%)
|
|
Patients with renal impairment
|
89
|
|
Patients with hepatic impairment
|
72
|
|
Elderly patients (Above 75 years)
|
79
|
|
Frail patients (Weight <60 kg)
|
79
|
|
Patients at high risk of bleeding
|
81
|
|
Patients with high CHA2DS2-VASc score
|
65
|
|
Patients with recurrent stroke
|
67
|
|
Patients with compliance issues on multiple medications
|
54
|
|
Patients with cost concern
|
51
|
|
Patients with concomitant IHD
|
58
|
|
Patients with a previous history of GI bleed
|
81
|
|
Patients with underlying malignancy
|
72
|
|
Consensus statement 6
Apixaban can be the preferred NOAC for primary and secondary stroke prophylaxis in Indian patients with AF, patients with history of GI bleed and underlying malignancy, the elderly and frail patients and those with hepatic or renal insufficiency and high risk of bleeding.
|
DISCUSSION
Atrial fibrillation is the most common chronic arrhythmia in clinical practice, which is associated with a well-known increased thromboembolic risk. It is a supraventricular tachyarrhythmia characterized by uncoordinated atrial activation with consequent deterioration of atrial mechanical function.39 The prevalence of AF is currently increasing owing to the longevity of the population globally. AF is independently associated with increased morbidity and mortality, including ischemic stroke, dementia, cognitive dysfunction, HF, MI and all-cause mortality.6
Early identification of the patients at risk of stroke can help in the primary prevention of stroke. The 2020 ESC guidelines of AF recommend opportunistic screening for AF in hypertensive patients and opportunistic screening for AF in patients with OSA.16 Oral anticoagulation represents the cornerstone of treatment to reduce the risk of cardioembolic stroke in patients with AF (Class of recommendation I, level of evidence A).26
The use of OACs is well-established in AF. Oral anticoagulant therapy reduces this risk by 62%.40 NOACs are now recommended as the first drug of choice as an alternative or in preference to warfarin in the American Heart Association/American College of Cardiology/Heart Rhythm Society (AHA/ACC/HRS) and the ESC guidelines for AF management, respectively. These drugs do not require INR monitoring or frequent dose adjustment and are associated with fewer food and drug interactions than VKAs.32
But, in the absence of head-to-head comparisons between different NOACs, making the choice of the NOAC most appropriate for the patient poses a clinical dilemma to the clinician. Several retrospective studies based on patient databases have brought forth the efficacy and safety of different NOACs in different patient populations. The current expert recommendations made using the DELPHI method can help in answering some of the clinical questions unanswered by current clinical trials.
The expert group supported the use of apixaban in elderly patients, patients with a high risk of bleeding, patients with comorbid disease and patients at high risk of stroke. These opinions corroborated the findings of the ARISTOTLE trial of apixaban, where apixaban demonstrated consistent benefits across NVAF patients with a wide range of stroke risks vs. warfarin (CHAD2DS2-VASc score 1, 2, ≥3 and HAS-BLED scores).41 The benefits of apixaban vs. warfarin were consistent in patients with AF regardless of age. Owing to the higher risk at an older age, the absolute benefits of apixaban were greater in the elderly.30 Apixaban treatment reduced the rate of stroke, death and major bleeding, regardless of renal function. Patients with impaired renal function seemed to have the greatest reduction in major bleeding with apixaban.42 Apixaban benefits were observed in patients with NVAF regardless of prior VKA treatment.43 The effects of apixaban versus warfarin were consistent in patients with AF with and without previous stroke or TIA. Owing to the higher risk of these outcomes in patients with previous stroke or TIA, the absolute benefits of apixaban might be greater in this population.42
The rates of stroke/systemic embolism and major bleeding were numerically lower among the patients assigned to apixaban, irrespective of prior VKA use.44 Apixaban demonstrated consistent benefits across NVAF patients with mild to moderate renal impairment versus warfarin.43 The AUGUSTUS trial findings supported the use of apixaban and a P2Y12 inhibitor without aspirin for most patients with AF and acute coronary syndrome and/or percutaneous coronary intervention, irrespective of a patient’s baseline bleeding and stroke risk.45
CONCLUSION
Atrial fibrillation is the most frequent cardiac arrhythmia. In AF, NOACs offer significant benefits for the prevention of stroke balanced by safety. Lower risks of death and bleeding with NOACs have been reported in meta-analyses of controlled trials. In elderly patients and in patients with a high risk of bleeding, apixaban is the preferred NOAC. In other populations, there are no distinct differences between the NOACs in terms of prevention of stroke.
Authorship
All named authors take the responsibility for the integrity of the work as a whole and have given their approval for this version to be published. The details published herein are intended for discrimination of educational, academic and/or research purposes and are not intended as a substitute for professional medical advice, diagnosis or treatment.
Compliance with Ethics Guidelines
This article has been developed as per the expert group consensus based on available literature and clinical experience. It does not contain any studies with human participants or animals performed by any of the authors.
Conflict of Interest: None.
|
List of Authors
|
|
Name
|
Designation
|
|
Ponde CK
|
Head, Dept. of Cardiology, Hinduja Hospital, Mumbai, Maharashtra, India
|
|
Shah VT
|
Consultant Cardiologist, Somaiya Hospital, Mumbai, Maharashtra, India
|
|
Shah Dhiren
|
Consultant Cardiologist, Wockhardt Hospital, Mumbai, Maharashtra, India
|
|
Khan Aziz
|
Director, Crescent Hospital, Nagpur, Maharashtra, India
|
|
Verma Gaurav
|
Head, Dept. of Cardiology, SMBT Hospital, Nashik, Maharashtra, India
|
|
Kochhar Arun
|
Professor and Head, Dept. of Cardiology, Fortis Hospital, Mohali, Chandigarh, India
|
|
Mahonan PP
|
Head, Dept. of Cardiology, Westfort Hi-Tech Hospital, Thrissur, Kerala, India
|
|
Dave Tarun
|
Consultant, Rajasthan Hospital & Jivraj Mehta Hospital, Ahmedabad, Gujarat, India
|
|
Dwivedi Shailendra
|
Head, Dept. of Cardiology, Jupiter Vishesh Hospital, Indore, Madhya Pradesh, India
|
|
Narayana Murthy
|
Consultant, Sagar Hospital, Bengaluru, Karnataka, India
|
|
John Satish
|
Head, Dept. of Cardiology, NRI Hospital, Vijayawada, Andhra Pradesh, India
|
|
Routray SN
|
Professor and Head, Dept. of Cardiology, SCB Medical College & Hospital, Cuttack, Odisha, India
|
|
Hazra PK
|
Head, Dept. of Cardiology, AMRI Hospitals, Kolkata, West Bengal, India
|
|
Bhadury Spandan
|
Professor and Head, Dept. of Cardiology, North Bengal Medical College & Hospital, Siliguri, West Bengal, India
|
|
Kuladhipati Indra
|
Chief Interventional Cardiologist, Downtown Hospital, Guwahati, Assam, India
|
|
Sharma AD
|
Medical Affairs, Alkem Laboratories Ltd., Mumbai, Maharashtra, India
|
|
Mayabhate MM
|
Medical Affairs, Alkem Laboratories Ltd., Mumbai, Maharashtra, India
|
|
Pawar DB
|
Medical Affairs, Alkem Laboratories Ltd., Mumbai, Maharashtra, India
|
REFERENCES
- Lippi G, Sanchis-Gomar F, Cervellin G. Global epidemiology of atrial fibrillation: an increasing epidemic and public health challenge. Int J Stroke. 2021;16(2):217-21.
- Heijman J, Sutanto H, Crijns HJ, Nattel S, Nattel S, Trayanova NA. Computational models of atrial fibrillation: achievements, challenges, and perspectives for improving clinical care. Cardiovasc Res. 2021;117(7):1682-99.
- Jame S, Barnes G. Stroke and thromboembolism prevention in atrial fibrillation. Heart. 2020;106(1):10-7.
- Migdady I, Russman A, Buletko AB. Atrial fibrillation and ischemic stroke: a clinical review. Semin Neurol. 2021;41(4):348-64.
- Healey JS, Amit G, Field TS. Atrial fibrillation and stroke: how much atrial fibrillation is enough to cause a stroke? Curr Opin Neurol. 2020;33(1):17-23.
- Brandes A, Smit MD, Nguyen BO, Rienstra M, Van Gelder IC. Risk factor management in atrial fibrillation. Arrhythm Electrophysiol Rev. 2018;7(2):118-27.
- Westermann D, Schrage B. Mitral stenosis and atrial fibrillation. Heart. 2020;106(10):713.
- Staerk L, Sherer JA, Ko D, Benjamin EJ, Helm RH. Atrial fibrillation: epidemiology, pathophysiology, and clinical outcomes. Circ Res. 2017;120(9):1501-17.
- Linz D, Nattel S, Kalman JM, Sanders P. Sleep apnea and atrial fibrillation. Card Electrophysiol Clin. 2021;13(1):87-94.
- Pistoia F, Sacco S, Tiseo C, Degan D, Ornello R, Carolei A. The epidemiology of atrial fibrillation and stroke. Cardiol Clin. 2016;34(2):255-68.
- Lane DA, Lip GY. Use of the CHA(2)DS(2)-VASc and HAS-BLED scores to aid decision making for thromboprophylaxis in nonvalvular atrial fibrillation. Circulation. 2012;126(7):860-5.
- Ronsoni RM, Saffi MAL, Gonçalves MVM, Nakayama IH, Luz Leiria TLL. A new vision at the interface of atrial fibrillation and stroke. Front Cardiovasc Med. 2021;8:689313.
- Baalman SWE, Boersma LVA, Allaart CP, Meine M, Scheerder COS, de Groot JR. Silent atrial fibrillation in patients with an implantable cardioverter defibrillator and coronary artery disease (INDICO AF) trial: Study rationale and design. Neth Heart J. 2018;26(12):628-33.
- Hagerty T, Rich MW. Fall risk and anticoagulation for atrial fibrillation in the elderly: a delicate balance. Cleve Clin J Med. 2017;84(1):35-40.
- da Silva Atrial fibrillation: epidemiology and peculiarities in the elderly. Cardiovasc Hematol Agents Med Chem. 2015;13(2):72-7.
- Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al; ESC Scientific Document Group. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42(5):373-498.
- Sharma M, Masih R, Mascarenhas DAN. Do all patients with atrial fibrillation need long-term anticoagulation? Clin Pract. 2017;7(3):955.
- Chao TF, Nedeljkovic MA, Lip GYH, Potpara TS. Stroke prevention in atrial fibrillation: comparison of recent international guidelines. Eur Heart J Suppl. 2020;22(Suppl O):O53-O60.
- Özge Mert G, Kepez A, Ugur Mert K, Görenek B. What to do with device-detected atrial high-rate episodes: Summary of the evidences. Pacing Clin Electrophysiol. 2022;45(2):250-61.
- Khan AA, Boriani G, Lip GYH. Are atrial high rate episodes (AHREs) a precursor to atrial fibrillation? Clin Res Cardiol. 2020;109(4):409-16.
- Benezet-Mazuecos J, Rubio JM, Farré J. Atrial high rate episodes in patients with dual-chamber cardiac implantable electronic devices: unmasking silent atrial fibrillation. Pacing Clin Electrophysiol. 2014;37(8):1080-6.
- Erküner Ö, Rienstra M, Van Gelder IC, Schotten U, Crijns HJGM, Luermans JGLM. Stroke risk in patients with device-detected atrial high-rate episodes. Neth Heart J. 2018;26(4):177-81.
- Almqvist M, Mattsson G, Magnusson P. Apparatdetekterad förmakstakykardi ökar risken för stroke – Riktlinjer saknas för behandling med antikoagulantia – europeiska rekommendationer ger vägledning [Device-detected atrial arrhythmia - when is anticoagulation indicated?]. Lakartidningen. 2019;116:FMHE.
- Shanmugam N, Boerdlein A, Proff J, Ong P, Valencia O, Maier SK, et al. Detection of atrial high-rate events by continuous home monitoring: clinical significance in the heart failure-cardiac resynchronization therapy population. Europace. 2012;14(2):230-7.
- Guo Y, Imberti JF, Kotalczyk A, Wang Y, Lip GYH; ChiOTEAF Registry Investigators. 4S-AF scheme and ABC pathway guided management improves outcomes in atrial fibrillation patients. Eur J Clin Invest. 2022;52(6):e13751.
- Cavallari I, Patti G. Efficacy and safety of oral anticoagulation in elderly patients with atrial fibrillation. Anatol J Cardiol. 2018;19(1):67-71.
- Robert-Ebadi H, Righini M. Anticoagulation in the elderly. Pharmaceuticals (Basel). 2010;3(12):3543-69.
- Schäfer A, Flierl U, Berliner D, Bauersachs J. Anticoagulants for stroke prevention in atrial fibrillation in elderly patients. Cardiovasc Drugs Ther. 2020;34(4):555-68.
- Deltour S, Pautas E. Anticoagulation decisions in elderly patients with stroke. Rev Neurol (Paris). 2020;176(9):692-700.
- Halvorsen S, Atar D, Yang H, De Caterina R, Erol C, Garcia D, et al. Efficacy and safety of apixaban compared with warfarin according to age for stroke prevention in atrial fibrillation: observations from the ARISTOTLE trial. Eur Heart J. 2014;35:1864-72.
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, et al; ESC Scientific Document Group. 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016;37(38):2893-962.
- January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC Jr, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines and the Heart Rhythm Society in collaboration with the Society of Thoracic Surgeons. Circulation. 2019;140(2):e125-51.
- Hammersley D, Signy M. Navigating the choice of oral anticoagulation therapy for atrial fibrillation in the NOAC era. Ther Adv Chronic Dis. 2017;8(12):165-76.
- Gupta N, Haft JI, Bajaj S, Samuel A, Parikh R, Pandya D, et al. Role of the combined CHADS2 score and echocardiographic abnormalities in predicting stroke in patients with paroxysmal atrial fibrillation. J Clin Neurosci. 2012;19(9):1242-5.
- Gundlund A, Staerk L, Fosbøl EL, Gadsbøll K, Sindet-Pedersen C, Bonde AN, et al. Initiation of anticoagulation in atrial fibrillation: which factors are associated with choice of anticoagulant? J Intern Med. 2017;282(2):164-74.
- Eikelboom JW, Wallentin L, Connolly SJ, Ezekowitz M, Healey JS, Oldgren J, et al. Risk of bleeding with 2 doses of dabigatran compared with warfarin in older and younger patients with atrial fibrillation: an analysis of the Randomized Evaluation of Long-term Anticoagulant Therapy (RE-LY) trial. Circulation. 2011;123(21):2363-72.
- Park S, Je NK. Factors influencing the selection of non-vitamin K antagonist oral anticoagulants for stroke prevention in patients with non-valvular atrial fibrillation. J Cardiovasc Pharmacol Ther. 2021;26(6):656-64.
- Joglar JA, Chung MK, Armbruster AL, Benjamin EJ, Chyou JY, Cronin EM, et al. 2023 ACC/AHA/ACCP/HRS Guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2023;148:e00-e00.
- Lip GY, Tello-Montoliu A. Management of atrial fibrillation. Heart. 2006;92(8):1177-82.
- Rockson SG, Albers GW. Comparing the guidelines: anticoagulation therapy to optimize stroke prevention in patients with atrial fibrillation. J Am Coll Cardiol. 2004;43(6):929-35.
- Lopes RD, Al-Khatib SM, Wallentin L, Yang H, Ansell J, Bahit MC, et al. Efficacy and safety of apixaban compared with warfarin according to patient risk of stroke and of bleeding in atrial fibrillation: a secondary analysis of a randomised controlled trial. Lancet. 2012;380(9855):1749-58.
- Easton JD, Lopes RD, Bahit MC, Wojdyla DM, Granger CB, Wallentin L, et al. ARISTOTLE Committees and Investigators. Apixaban compared with warfarin in patients with atrial fibrillation and previous stroke or transient ischaemic attack: a subgroup analysis of the ARISTOTLE trial. Lancet Neurol. 2012;11(6):503-11.
- Hohnloser SH, Hijazi Z, Thomas L, Alexander JH, Amerena J, Hanna M, et al. Efficacy of apixaban when compared with warfarin in relation to renal function in patients with atrial fibrillation: insights from the ARISTOTLE trial. Eur Heart J. 2012;33(22):2821-30.
- Garcia DA, Wallentin L, Lopes RD, Thomas L, Alexander JH, Hylek EM, et al. Apixaban versus warfarin in patients with atrial fibrillation according to prior warfarin use: results from the Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation trial. Am Heart J. 2013;166(3):549-58.
- Harskamp RE, Fanaroff AC, Lopes RD, Wojdyla DM, Goodman SG, Thomas LE, et al. Antithrombotic therapy in patients with atrial fibrillation after acute coronary syndromes or percutaneous intervention. J Am Coll Cardiol. 2022;79(5):417-27.
|