Published in IJCP
February 2024
Clinical Study
Post-Traumatic Renal Artery Pseudoaneurysm Managed Successfully with Angioembolization
February 10, 2024 | Keyur Patel, Rajendra B Nerli, Navin Mulimani, Shreyas Rai, Abhinay Jogula, Ashwin Bokare, Nishant Setya
Nephrology
Abstract
Introduction: Renal artery pseudoaneurysm is a rare complication of blunt renal trauma. Super-selective angioembolization is a minimally invasive, effective procedure to manage traumatic renal artery pseudoaneurysm, in patients who are hemodynamically stable. We report our experience in the management of patients with post-traumatic bleeding pseudoaneurysm with angioembolization. Materials and methods: We retrospectively reviewed the inpatient and outpatient records and imaging data of our hospital, of all patients with history of blunt injury to kidneys, admitted with massive hematuria and underwent angioembolization to control the bleeding. Results: During the study period, 3 patients (all male) with a mean age of 26.66 years presented to us with blunt injury abdomen. Contrast computed tomography (CT) revealed Grade IV renal injury in 2 patients and Grade V injury in 1 patient. Focal intensively enhancing areas were noted at the site of renal parenchymal lacerations suggestive of pseudoaneurysms. Super-selective catheterization was performed and embolization done using 50% N-butyl-2-cyanoacrylate (NBCA) + Lipiodol. Conclusions: Angioembolization, a radiographic intervention, is an effective and minimally invasive technique to stop active bleeding from renal artery pseudoaneurysms.
Keywords: Delayed hematuria, blunt renal trauma, minimally invasive technique
Over the last few decades, there has been a clear transition towards a nonoperative approach in the management of renal trauma.1-3 A combination of several factors has probably led to this transition namely i) the accumulated knowledge about the safety and outcome of the nonoperative approach in renal trauma; ii) improvement in imaging modalities such as computed tomography (CT)4 and iii) advances in minimally invasive treatment techniques such as angioembolization in cases of active bleeding,5,6 and endourological stenting in cases of urine extravasation.7,8
As per the current guidelines (American Urological Association [AUA]9 and European Association of Urology [EAU]10), the absolute indications for renal intervention include hemodynamic instability unresponsive to aggressive resuscitation secondary to renal hemorrhage, Grade V vascular injuries and an expanding or pulsatile perirenal hematoma identified at the time of laparotomy performed for associated injuries. Relative indications for renal intervention include11 a large laceration of the renal pelvis, avulsion of the ureteropelvic junction (UPJ), co-existing bowel or pancreatic injuries, persistent urinary leakage and post-injury urinoma or perinephric abscess with failed percutaneous or endoscopic management. Nonoperative management includes observation with supportive care, bed rest with monitoring of vital signs and laboratory tests and reimaging (whenever felt necessary or in cases of deterioration), with the appropriate use of minimally invasive procedures (angioembolization or ureteral stenting) whenever indicated.
Complications following renal trauma usually depend on the grade of the initial renal injury and the method of management.12 The resulting complications are usually of minimal long-term morbidity, that can be successfully managed using end urologic and percutaneous techniques, and do not significantly prolong the mean days of hospitalization.13,14 Early complications are those that occur within 1 month of injury, and include urinoma, delayed bleeding, urinary fistula, abscess and hypertension. Prolonged urinary extravasation is the most common complication after renal trauma.13,15 Delayed renal bleeding most commonly occurs within 2 weeks of injury. When bleeding is heavy or symptomatic, transfusions, angiography and super-selective embolization may be required.16 Herein, we report our experience in the management of patients with post-traumatic bleeding pseudoaneurysm with angioembolization.
MATERIALS AND METHODS
We retrospectively reviewed the inpatient and outpatient records including imaging data of our hospital, of all patients with history of blunt injury to kidneys who were admitted with massive hematuria and underwent angioembolization to control bleeding.
Ethical Considerations: The protocol of the study was approved by Ethics Committee of the Institute. The design and objectives of the study were explained and a written permission obtained from the Ethical Committee.
RESULTS
During the study period, from July 2015 to June 2021, 3 patients (all male) with a mean age of 26.66 years presented to us with blunt injury abdomen. Fall from a two-wheeler, collapse of wall and being hit by a four-wheeler were the causes of trauma. All 3 had received primary care at a local hospital and were managed conservatively. They were referred to our hospital for delayed bleeding (hematuria) at a mean duration of 23 days after trauma. All the 3 patients appeared pale and had low hemoglobin values as seen in Table 1.
|
Table 1. Details of Patient Demographics
|
|
Age (years)
|
Gender
|
Renal injury
|
Other abdominal injuries
|
Delayed bleeding
|
Hb (gm%)
|
|
18
|
M
|
Right Grade IV
|
Liver
|
21 days
|
7
|
|
33
|
M
|
Left Grade V
|
Mesentery
|
30 days
|
6.2
|
|
29
|
M
|
Left Grade IV
|
Spleen
|
18 days
|
8
|
|
26.66 (mean)
|
|
|
|
23 (mean)
|
|
Contrast CT (Fig. 1) done revealed Grade IV renal injury in 2 patients and Grade V injury in 1 patient. Focal intensely enhancing areas were noted at the site of renal parenchymal lacerations suggestive of pseudoaneurysms. Perirenal collection was also noted. In view of the persistent bleeding and presence of pseudoaneurysms, the patients were counseled for complete endovascular embolization.
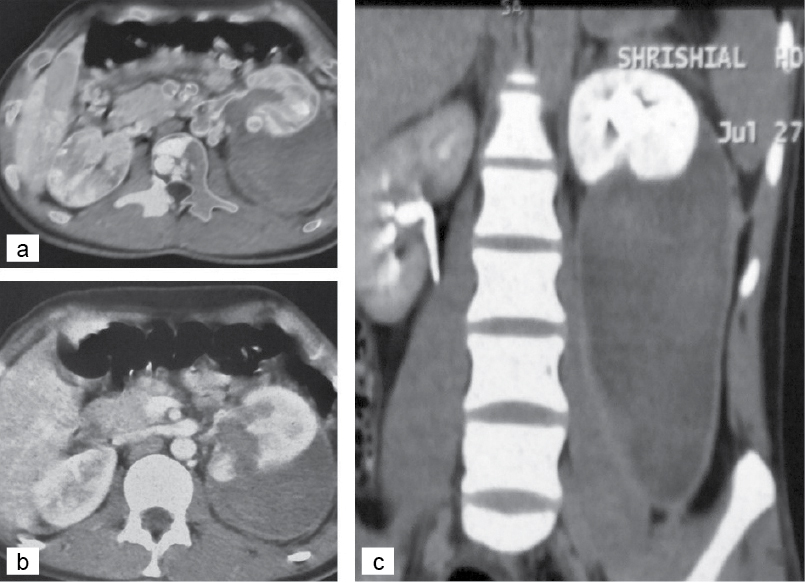
Figure 1. (a) CT scan showing a huge perirenal collection. (b) scan showing lower polar laceration communicating with renal pelvis. (c) CT scan showing a huge perirenal collection trickling down the fascia of Gerota.
The embolization procedure was performed under local anesthesia. Retrograde Seldinger technique was utilized through the opposite femoral arterial access. A diagnostic renal angiogram was performed using a Cobra catheter. Once the pseudoaneurysm was confirmed, the 5 Fr Cobra catheter and Progreat catheter were used to perform super-selective catheterization and embolization using 50% N-butyl-2-cyanoacrylate (NBCA) + Lipiodol (Fig. 2). Check angiogram of the renal artery showed complete embolization of the pseudoaneurysm with normal opacification of the rest of the renal arterial branches.
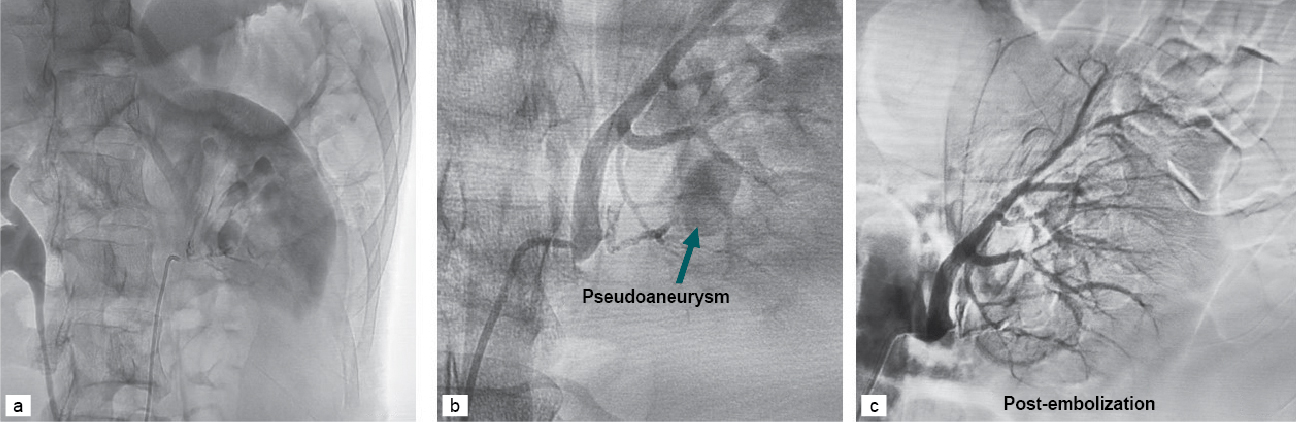
Figure 2. (a and b) Diagnostic renal angiogram showing a pseudoaneurysm involving the lower pole. (c) Post-embolization renal angiogram.
The post-embolization period was uneventful. Patients were discharged after 72 hours and were followed up for at least 12 months after embolization.
DISCUSSION
Blunt trauma remains the most common cause of renal injuries (90%) and only 10% to 15% of these can be classified as major injuries.17 Renovascular injuries, such as transection, thrombosis, dissection and arteriovenous fistula formation are well-recognized but rare consequences of blunt renal trauma.18,19 Renal artery pseudoaneurysms usually result after iatrogenic renal procedures, although they can also occur as a rare complication of blunt renal trauma.19,20 Renal artery pseudoaneurysm is believed to result from rapid deceleration-induced, full- or partial-thickness injury to arteries supplying the renal parenchyma.18,20,21 Following complete or partial injury of an artery, blood seeps through the surrounding tissues namely vascular adventitia, renal parenchyma and Gerota’s fascia.
Temporary cessation of bleeding occurs immediately after the injury due to hypotension and local coagulation. As the clot undergoes lysis and the surrounding necrotic tissue degrades, it results in recanalization between the intravascular and extravascular spaces and, subsequently, the formation of a pseudoaneurysm. Restoration of normal blood flow and pressure, leads to the growth of the pseudoaneurysm, which eventually ruptures into the pyelocalyceal system or the perirenal space.18,20,22 Gross hematuria from blunt parenchymal injury, typically resolves within several hours and can be effectively managed with bed rest and transfusion support, until the urine clears and vital signs are stable. However, persistent bleeding or delayed gross hematuria should raise the suspicion of segmental vascular injury, including pseudoaneurysm formation and prompt further investigation and management.19-21
In broad terms, it is preferable to use noninvasive techniques or strategies such as angioembolization for cases of persistent bleeding in hemodynamically stable patients. Breyer et al23 suggested a treatment algorithm, which complements the current AUA guidelines for management of renal trauma.9 A contrast-enhanced CT imaging with delayed and immediate phases is the first step that would provide the grade of renal trauma as well as help into visualize the renal arteries, veins and parenchyma. Primary angioembolization interventions are ideally suited for patients with persistent bleeding, and an intact main renal artery and vein. All patients managed conservatively for renal trauma should be monitored and observed for a change in hemodynamic status, as delayed hemorrhage is known to occur from a pseudoaneurysm.20,22 Figure 3 depicts an algorithm for the management of renal trauma. A prospective study found that 18% of those treated with nonoperative intent ultimately needed surgical intervention.24 In these cases of delayed hemorrhage, angioembolization is a good first-line choice of treatment.
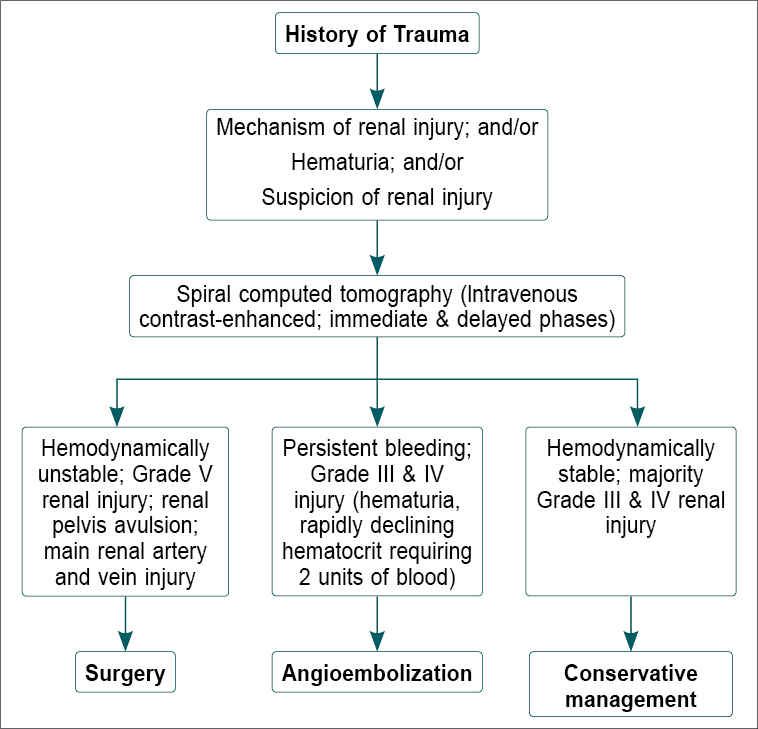
Figure 3. Flowchart showing management of renal trauma.
CONCLUSION
Renal artery pseudoaneurysm formation following a blunt abdominal trauma is rare. However, whenever there is delayed gross hematuria, the possibility of pseudoaneurysm should be considered, and managed by angioembolization.
Conflict of Interest: None.
REFERENCES
- Nerli RB, Metgud T, Patil S, Guntaka A, Umashankar P, Hiremath M, et al. Severe renal injuries in children following blunt abdominal trauma: selective management and outcome. Pediatr Surg Int. 2011;27(11):1213-6.
- Erlich T, Kitrey ND. Renal trauma: the current best practice. Ther Adv Urol. 2018;10(10):295-303.
- Nerli RB, Ghagane SC, Musale A, Mungarwadi A, Dixit NS, Hiremath MB. High grade renal trauma in a child with rupture bladder and fracture pelvic bones. Urol Case Ref. 2019;24:100850.
- Santucci RA, Fisher MB. The literature increasingly supports expectant (conservative) management of renal trauma - a systematic review. J Trauma. 2005;59(2):493-503.
- Hotaling JM, Sorensen MD, Smith TG 3rd, Rivara FP, Wessells H, Voelzke BB. Analysis of diagnostic angiography and angioembolization in the acute management of renal trauma using a national data set. J Urol. 2011;185(4):1316-20.
- Shankar K. Delayed severe bleeding following partial nephrectomy managed with selective embolization: a case report. J Nephrol Urol. 2022;6(4).
- Alsikafi NF, McAninch JW, Elliott SP, Garcia M. Nonoperative management outcomes of isolated urinary extravasation following renal lacerations due to external trauma. J Urol. 2006;176(6 Pt 1):2494-7.
- Haas CA, Reigle MD, Selzman AA, Elder JS, Spirnak JP. Use of ureteral stents in the management of major renal trauma with urinary extravasation: is there a role? J Endourol. 1998;12(6):545-9.
- Morey AF, Brandes S, Dugi DD 3rd, Armstrong JH, Breyer BN, Broghammer JA, et al; American Urological Assocation. Urotrauma: AUA guideline. J Urol. 2014;192(2):327-35.
- Kitrey ND, Djakovic N, Gonsalves M, et al. EAU guidelines on urological trauma. 2017;8-17.
- Santucci RA, Wessells H, Bartsch G, Descotes J, Heyns CF, McAninch JW. Evaluation and management of renal injuries: consensus statement of the renal trauma subcommittee. BJU Int. 2004;93(7):937-54.
- Bryant WK, Shewakramani S. Emergency management of renal and genitourinary trauma: best practices update. Emerg Med Pract. 2017;19(8):1-20.
- Lee WJ, Smith AD, Cubelli V, Badlani GH, Lewin B, Vernace F, et al. Complications of percutaneous nephrolithotomy. AJR Am J Roentgenol. 1987;148(1):177-80.
- Peterson NE. Intermediate-degree blunt renal trauma. J Trauma. 1977;17(6):425-35.
- Fukumori T, Yamamoto A, Ashida S, Komatsu F, Matsumoto S, Yuasa K. Extracorporeal shock wave lithotripsy-induced renal laceration. Int J Urol. 1997;4(4):419-21.
- Hardeman SW, Husmann DA, Chinn HK, Peters PC. Blunt urinary tract trauma: identifying those patients who require radiological diagnostic studies. J Urol. 1987;138(1):99-101.
- Halachmi S, Chait P, Hodapp J, Bgli DG, McLorie GA, Khoury AE. Renal pseudoaneurysm after blunt renal trauma in a pediatric patient: management by angiographic embolization. Urology. 2003;61(1):224.
- Swana HS, Cohn SM, Burns GA, Egglin TK. Renal artery pseudoaneurysm after blunt abdominal trauma: case report and literature review. J Trauma. 1996;40(3):459-61.
- Heyns CF, Stellmacher GA. Selective renal artery embolization in the management of non-iatrogenic renal trauma – experience in 28 patients. African J Urol. 2005;11(2):89-94.
- Miller DC, Forauer A, Faerber GJ. Successful angioembolization of renal artery pseudoaneurysms after blunt abdominal trauma. Urology. 2002;59(3):444.
- Jebara VA, El Rassi I, Achouh PE, Chelala D, Tabet G, Karam B. Renal artery pseudoaneurysm after blunt abdominal trauma. J Vasc Surg. 1998;27(2):362-5.
- Lee DG, Lee SJ. Delayed hemorrhage from a pseudoaneurysm after blunt renal trauma. Int J Urol. 2005;12(10):909-11.
- Breyer BN, McAninch JW, Elliott SP, Master VA. Minimally invasive endovascular techniques to treat acute renal hemorrhage. J Urol. 2008;179(6):2248-52; discussion 2253.
- Lanchon C, Fiard G, Arnoux V, Descotes JL, Rambeaud JJ, Terrier N, et al. High grade blunt renal trauma: predictors of surgery and long-term outcomes of conservative management. A prospective single center study. J Urol. 2016;195(1):106-11.
|