Abstract
Introduction: Patients with human immunodeficiency virus and acquired immunodeficiency syndrome (HIV/AIDS) are prone to opportunistic infections (OIs) given their immunosuppressed state. OIs continue to cause morbidity and mortality in HIV/AIDS patients even after highly-active antiretroviral therapy (HAART); hence, attainment of the goals on health care programs, particularly in resource-poor countries, is hard to achieve. The prevalence of specific OIs varies in different countries and even in different areas within the same country. Little information is available about the prevalence of OI in HIV patients from developing countries, especially India. Early diagnosis and prompt treatment contribute to increased life expectancy among infected patients delaying progression to AIDS. Hence, the present study was carried out to elucidate current frequencies and spectrum of OIs in HIV seropositive adult patients in Haryana and to evaluate the associated risk factors for OIs. Materials and methods: This was a cross-sectional study carried out at the Dept. of General Medicine in a tertiary care hospital in North India. Basic demographic details, anthropometric measurements, symptoms of HIV/OI, clinical examination, biochemical investigations and treatment details were recorded. Patients aged 18 to 70 years and HIV seropositive subjects were included in the study. Results: The study found that about 53.21% of HIV/AIDS patients on ART had one or more OIs. Tuberculosis (TB) was the predominant OI identified, with a prevalence of 25.71%. Candidiasis and herpes zoster were the second and the third most prevalent OIs at 13.8% (101/731) and 7.25% (53/731), respectively. Age (43.4 ± 10.7 years), low income, illiteracy, low socioeconomic status, initial 4 months since initiation of ART, CD4 count <200/mm3, body mass index of <18.5 kg/m², poor ART adherence, hemoglobin, albumin were strongly associated with OIs. Conclusion: The present study shows that TB is the commonest OI in adults and the overall population of people living with HIV (PLHIV) in Haryana and proves that OIs across different patient groups vary significantly. Various factors like adherence to HAART, socioeconomic and education status of patients can influence the occurrence and outcome of these deadly infections.
Keywords: Spectrum, opportunistic infections, PLHIV
Human immunodeficiency virus (HIV) infection is one of most studied infectious diseases since it was first recognized clinically in 1981 in the United States of America. HIV-related opportunistic infections (OIs) have been defined as infections that are more frequent or more severe because of HIV-mediated immunosuppression.1 OIs are the first clinical manifestations that alert clinicians to the occurrence of the acquired immunodeficiency syndrome (AIDS). These OIs occurs on average 7 to 10 years after infection with HIV.2,3 Until effective antiretroviral therapy (ART) was developed, patients generally survived for only 1 to 2 years after the initial manifestation of AIDS.4 However, OIs continue to cause morbidity and mortality in HIV/AIDS patients even after highly-active antiretroviral therapy (HAART); hence, the attainment of the goals on health care programs, particularly in resource-poor countries, is hard to achieve. OIs shorten the life span of people with HIV infection and require expensive treatments, which carry a substantial financial burden, especially for a developing country like India. Timely intervention helps HIV-positive persons live longer and also helps to prevent transmission in the community.5
Estimating the cost of necessary health care as accurately as possible must be the first step in planning specialized health services, which is only possible if we know how the OIs are distributed in a given place. Also, there is no denying that HIV-related OIs affect a person’s quality of life and contributes to the overall disability-adjusted life years (DALY) caused by AIDS. The prevalence of specific OIs varies in different countries and even in other areas within the same country. Identifying such OIs is especially important for HIV and AIDS case management. Little information is available about the prevalence of OI in HIV patients from developing countries, especially India. Early diagnosis of OIs and prompt treatment contribute to increased life expectancy among infected patients delaying progression to AIDS. Hence, this study was carried out to elucidate current prevalence and spectrum of OIs infecting HIV-seropositive adult patients in Haryana, a northern state in India, and to evaluate the associated risk factors of OIs. Identifying such pathogens is very important for clinicians and health planners to tackle the AIDS epidemic more effectively.
MATERIALS AND METHODS
This was a cross-sectional study carried out at a tertiary care center in North India. Adult patients between 18 to 70 years attending the Nodal ART Centre, admitted under Dept. of Medicine PGIMS, Rohtak, Haryana, and admitted under clinics were enrolled in this study. Patients who did not consent to participate in the study, those with psychiatric illness taking regular medications, pregnant and lactating mothers, those with non-HIV/AIDS-related malignancy, known cases of chronic kidney and liver disease prior to diagnosis of HIV and patients with an altered sensorium or cognitive impairment severely affecting communication were excluded from the study. Our Nodal ART Centre has all the adequate facilities and investigations for detecting the OI before commencing ART.
Detailed information of all enrolled patients was filled in a proforma designed for the study purpose. This included basic demographic details, anthropometric measurements, symptoms of HIV/OI, clinical examination and treatment. At baseline, each patient underwent hematological and biochemical investigations. Patients were assessed for OI risk factors. These included age, weight at last visit, serum albumin at diagnosis of OI, World Health Organization (WHO) clinical stage III and IV, CD4 count at the time of diagnosis of OI, initiation of ART since diagnosis of HIV and adherence to ART. The Center for Adherence Support Evaluation (CASE) Adherence Index, a simple composite measure of self-reported ART adherence, was utilized to assess adherence to ART.6 Informed consent was taken from all participants and study was approved from ethical committee of the institute and Haryana state division of National AIDS Control Society.
The diagnosis of OI was made following standard guidelines where possible and facilities available. Where diagnosis was based on clinical grounds alone, the opinion of two independent physicians involved in enrolled patient care and management was required before such diagnosis was accepted.
Statistical Analysis
Statistical Package for Social Sciences (SPSS) Version 23 was used for all descriptive and statistical analysis. Association of OIs was done by subgroup analysis of WHO staging, CD4 count, demographic and biochemical/hematological profile and treatment adherence. The distribution of data was analyzed and appropriate parametric/nonparametric tests were used for statistical analysis. Continuous data were expressed as means ± standard deviation (SD), and the means were compared using a t-test. Nominal data were expressed as frequencies or proportions, and the Chi-square test and Fisher’s exact test were used to compare the differences in frequency. For all tests, a p-value of <0.05 will be considered significant, and the confidence interval will be kept at 95%.
RESULTS AND OBSERVATIONS
The study was conducted in the Dept. of General Medicine, PGIMS, Rohtak, Haryana, India. A total of 731 patients aged 18 to 70 years and HIV seropositive subjects were included in the study. The baseline characteristic of the study participants is presented in Table 1.
|
Table 1. Distribution of Demographic Characteristics of Study Subjects
|
|
Demographic characteristics
|
Frequency
|
Percentage (%)
|
|
Gender
Female
Male
Transgender
|
284
438
9
|
38.85
59.92
1.23
|
|
Area of residence
Rural
Urban
|
534
197
|
73.05
26.95
|
|
Religion
Christian
Hindu
Muslim
Sikh
|
3
717
10
1
|
0.41
98.08
1.37
0.14
|
|
Income
<2,000
2,000-5,000
5,001-20,000
>20,000
|
135
232
298
66
|
18.47
31.74
40.77
9.03
|
|
Socioeconomic status
Lower
Upper lower
Lower middle
Upper middle
Upper
|
51
113
377
120
70
|
6.98
15.46
51.57
16.42
9.58
|
|
Education
Illiterate
Primary school
Secondary school
College and Above
|
172
271
208
80
|
23.53
37.07
28.45
10.94
|
|
Marital status
Married
Unmarried
Widow/Widower
|
655
23
53
|
89.60
3.15
7.25
|
|
Spouse
Expired
Nonreactive
Reactive
|
52
289
198
|
9.65
53.62
36.73
|
|
Age (years)
Mean ± SD
Median (25th-75th percentile)
Range
|
40.02 ± 11.17
38 (32-48)
19-70
|
The study found that about 53.21% of HIV/AIDS patients had one or more OIs compared to 46.79% who had no OI. Tuberculosis (TB) (48.32% of total OIs) was the predominant OI identified, with a prevalence of 25.71% (200/731). Of these, 71.80% (n = 135/188) were pulmonary TB and 31.3% were extrapulmonary TB (n = 59/188). Among the extrapulmonary TB cases, 35 were abdominal TB and 24 were TB meningitis. Candidiasis and herpes zoster were the second and the third most prevalent OIs in the present study, at 13.8% (101/731) and 7.25% (53/731), respectively (Table 2).
|
Table 2. Distribution of Opportunistic Infections of Study Subjects
|
|
Opportunistic infections
|
Frequency
|
Percentage (%)
|
Percentage (%) from total OI
|
|
No OI
|
342
|
46.79
|
-
|
|
Skin
Herpes zoster
Kaposi sarcoma
|
73
53
20
|
9.99
7.25
2.74
|
18.77
13.62
5.14
|
|
CNS
TBM
Primary CNS lymphoma
PMLE
Cryptococcal meningitis
Cerebral toxoplasmosis
|
56
24
3
2
15
12
|
7.66
3.28
0.41
0.27
2.05
1.64
|
14.40
6.17
0.77
0.51
3.86
3.08
|
|
GIT
Abdominal TB
Chronic mucocutaneous candidiasis
Candidal esophagitis
HSV oral ulcers
|
166
35
100
1
16
|
22.71
4.79
13.68
0.14
2.19
|
42.67
9.00
25.71
0.26
4.11
|
|
Chronic diarrhea
Cryptosporidiosis
Giardiasis
Isosporiasis
Schistosomiasis
|
20
14
1
2
3
|
2.74
1.92
0.14
0.27
0.41
|
5.14
3.60
0.26
0.51
0.77
|
|
Respiratory
Pulmonary TB
|
161
135
|
22.02
18.47
|
41.39
34.70
|
|
Other bacterial
Klebsiella pneumoniae
Pseudomonas aeruginosa pneumonia
Streptococcus pneumoniae
|
12
3
1
8
|
1.64
0.41
0.14
1.09
|
3.08
0.77
0.26
2.06
|
|
Fungal
Aspergillus fumigatus pneumonia
Histoplasma capsulatum pneumonia
Cryptococcus neoformans pneumonia
Pneumocystis jirovecii pneumonia
|
8
1
1
1
5
|
1.09
0.14
0.14
0.14
0.68
|
2.06
0.26
0.26
0.26
1.29
|
|
Hematology
Diffuse large B-cell lymphoma
|
10
10
|
1.37
1.37
|
2.57
2.57
|
|
Eye
CMV retinitis
|
1
1
|
0.14
0.14
|
0.26
0.26
|
|
Total pulmonary and extrapulmonary
|
188
|
25.71
|
48.32
|
OI = Opportunistic infection; TB = Tuberculosis; CNS = Central nervous system; TBM = Tuberculosis meningitis; PMLE = Polymorphous light eruption; GIT = Gastrointestinal tract; HSV = Herpes simplex virus; CMV = Cytomegalovirus.
There were 63 co-infections of different OIs observed in the current study. Of these, 55 had 2 co-infections, 7 had 3 co-infections and 1 patient had 4 co-infections. TB with candidiasis were the most common co-infection (32 cases) followed by TB with cryptosporidiosis (4 cases).
The mean ± SD of age (years) in patients with OI was 43.4 ± 10.7, which was significantly higher than patients without OI (36.18 ± 10.43). The proportion of patients with OI was significantly higher in patients with income (in Rupees) (<2,000 [68.15.52%] and 2,000-5,000 [60.34%]) as compared to 5,000-20,000 (45.97%) and >20,000 (30.30%). OIs were significantly higher in illiterate people (66.86%) as compared to those with primary school education (52.40%), secondary school education (54.33%) and college and higher education (23.75%) with a p-value of <0.0001. It was found that 90.20% of patients in the lower Kuppuswamy class had OIs as compared to upper-lower (57.52%), lower-middle (52.25%), upper-middle (41.67%) and upper class (44.29%) with a p-value <0.0001. OIs were significantly higher in patients with body mass index (BMI) (kg/m²) of <18.5 (underweight; 83.94%) as compared to 18.5-24.99 (normal BMI; 44.23%), 25-29.99 (overweight; 3.85%), ≥30 (obese; 0%) with p value of <0.0001. Significant association was seen between weight (kg) and OIs. Mean ± SD of weight (kg) in patients without OI was 58.7 ± 9.17, which was significantly higher as compared to patients with OI (52.72 ± 7.21) with p value of <0.0001.
The proportion of patients with OI was significantly higher in time since ART initiation (months) ≤12 months (71.84%) as compared to 13 to 24 months (30.19%), 25 to 36 months (26.67%), 37 to 48 months (57.64%), 49 to 60 months (53.33%), 61 to 72 months (55.56%) and ≥73 months (52.21%) (p < 0.0001). The proportion of patients with OI was significantly higher within 1 to 4 months (83.33%) as compared to 5 to 8 months (66.67%), 9 to 12 months (50%) after HAART initiation with p value of 0.011. This signifies that as the viral load decreases and CD4 count improves, the risk of OIs reduces significantly.
The highest prevalence was seen in patients categorized as WHO clinical stage IV and III (n = 135/135, 100%) and (n = 193/193, 100%), respectively, while the lowest prevalence was observed among clinical stage I patients (n = 1/342, 0.29%). Statistically, a significant association was depicted between the prevalence of OIs and WHO clinical stages II, III and IV.
The prevalence of OIs was found to be highest (n = 225/225, 100%) among HIV-infected patients with CD4 count <200/mm3 followed by CD4 count 200-349/mm3 and count 350-499/mm3 with a prevalence of (n = 122/157, 77.71%) and (n = 30/127, 23.62%), respectively whereas, the prevalence was significantly lower in patients with CD4 count more than 500/mm3 with a prevalence of only 5.41% (Fig. 1). The mean ± SD CD4 count/mm³ in patients without OI was 600.37 ± 246.8, which was significantly higher than patients with OI (199.07 ± 116.88).
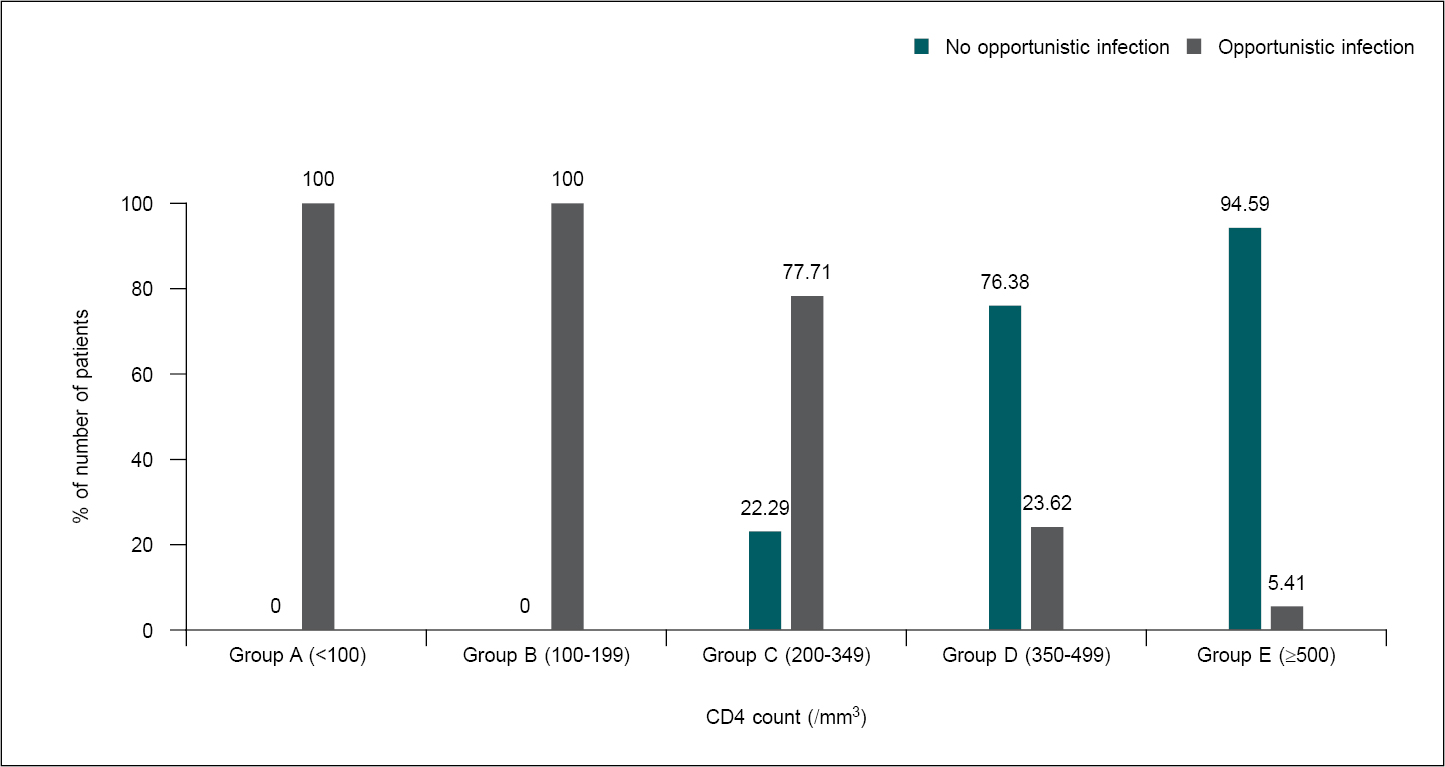
Figure 1. Association of CD4 count (/mm³) with opportunistic infection.
Good adherence to ART was seen in 503 (68.81%) patients, and poor adherence was present in 228 patients (31.19%). OIs were significantly higher in patients with poor ART adherence (99.12%) as compared to good adherence (32.41%).
A significant association was seen between low hemoglobin, protein (g/dL), albumin (g/dL) and OI. Mean ± SD protein (g/dL) and albumin (g/dL) in patients without OI was 7.51 ± 0.86, 3.9 ± 0.51, respectively, which was significantly higher as compared to patients with OI (7.29 ± 0.88 (p = 0.0006), 3.63 ± 0.6 (p < 0.0001)), respectively.
On univariate analysis, co-factors that had significant association with OIs were low-income education/socioeconomic status, age, weight/BMI, hemoglobin, albumin, CD4 count, WHO staging, adherence to ART (Table 3).
|
Table 3. Baseline Characteristics and Univariate and Multivariate Risk Factor Analysis for Opportunistic Infection
|
|
Characteristics
|
No OI (n = 342)
|
OI (n = 389)
|
Univariate analysis
|
Multivariate analysis
|
|
OR (95% CI)
|
P value
|
OR
|
P value
|
|
Age (years)
Mean ± SD
|
36.18 ± 10.43
|
43.39 ± 10.73
|
1.066 (1.05-1.082)
|
<0.0001
|
|
|
|
Income
<2,000
2,000-5,000
5,001-20,000
>20,000
|
43 (31.85%)
92 (39.66%)
161 (54.03%)
46 (69.70%)
|
92 (68.15%)
140 (60.34%)
137 (45.97%)
20 (30.30%)
|
1
0.714 (0.457-1.117)
0.4 (0.261-0.614)
0.207 (0.11-0.392)
|
<0.0001
|
|
|
|
Socioeconomic status
Lower
Upper lower
Lower middle
Upper middle
Upper
|
5 (9.80%)
48 (42.48%)
180 (47.75%)
70 (58.33%)
39 (55.71%)
|
46 (90.20%)
65 (57.52%)
197 (52.25%)
50 (41.67%)
31 (44.29%)
|
1
0.16 (0.061-0.42)
0.129 (0.052-0.323)
0.085 (0.032-0.222)
0.094 (0.034-0.259)
|
<0.0001
|
|
|
|
Education
Illiterate
Primary school
Secondary school
College and above
|
57 (33.14%)
129 (47.60%)
95 (45.67%)
61 (76.25%)
|
115 (66.86%)
142 (52.40%)
113 (54.33%)
19 (23.75%)
|
1
0.548 (0.368-0.815)
0.592 (0.389-0.899)
0.158 (0.086-0.288)
|
<0.0001
|
|
|
|
Weight (kg)
Mean ± SD
|
58.7 ± 9.17
|
52.72 ± 7.21
|
0.913 (0.895-0.932)
|
<0.0001
|
|
|
|
BMI (kg/m²)
18.5-24.99 (Normal)
<18.5 (Underweight)
25-29.99 (Overweight)
≥30 (Obese)
|
285 (55.77%)
31 (16.06%)
25 (96.15%)
1 (100%)
|
226 (44.23%)
162 (83.94%)
1 (3.85%)
0 (0%)
|
1
0.15 (0.101- 0.234)
0.01 (0.002-0.064)
0.06 (0.001-6.069)
|
<0.0001
|
|
|
|
WHO clinical staging
I
II
III
IV
|
341 (99.71%)
1 (1.64%)
0 (0%)
0 (0%)
|
1 (0.29%)
60 (98.36%)
193 (100%)
135 (100%)
|
1
9182.5 (929.2-90739.2)
88107 (3545.5-2189448.1)
61697.667
(2472.9-1539321.7)
|
<0.0001
|
1.000
20188.20
26264.03
116.37
|
<0.0001
<0.0001
0.050
|
|
CD4 count (/mm3)
Group A (<100)
Group B (100-199)
Group C (200-349)
Group D (350-499)
Group E (≥500)
|
0 (0%)
0 (0%)
35 (22.29%)
97 (76.38%)
210 (94.59%)
|
60 (100%)
165 (100%)
122 (77.71%)
30 (23.62%)
12 (5.41%)
|
1
2.73 (0.05-142.5)
0.029 (0.002-0.48)
0.003 (0-0.04)
0 (0-0.009)
|
<0.0001
|
0.98
|
0.02
|
|
Hemoglobin (g/dL)
|
12.51 ± 2.31
|
9.87 ± 1.83
|
0.56 (0.5-0.6)
|
<0.0001
|
|
|
|
ART adherence
Good adherence
Poor adherence
|
340 (67.59%)
2 (0.88%)
|
163 (32.41%)
226 (99.12%)
|
1
188.681 (53.3- 667.1)
|
<0.0001
|
-
913.992
|
-
0.0004
|
|
Albumin (g/dL)
|
3.9 ± 0.51
|
3.63 ± 0.6
|
0.412 (0.3-0.5)
|
<0.0001
|
|
|
On performing multivariate regression, CD4 count, low case adherence index score (poor adherence) and WHO staging (stage II, stage III and stage IV) were significant independent risk factors of OI after adjusting for confounding factors. Patients with low case adherence index score (poor adherence), WHO staging (stage II, stage III, stage IV) had significantly high risk of OI with adjusted odds ratio (OR) of 913.992 (21.282-39,252.803), 20.188.208 (678.408-60,0764.698), 26.264.032 (640.880-1076331.334), respectively. With the increase in CD4, risk of OI significantly decreased with adjusted OR of 0.989 (0.98-0.999) (Table 3).
DISCUSSION
HIV is a major global public health issue, which has claimed more than 40 million lives so far with ongoing transmission globally. Despite the availability of ART, it is not a 100% curable disease. OIs and associated complications account for considerable morbidity and mortality in people living with HIV (PLHIV). The present study involving 731 patients on ART was carried out to elucidate current frequencies and spectrum of OIs infecting HIV seropositive adult patients in Haryana and to evaluate the associated risk factors of OIs.
The most common self-reported risk factor for the occurrence of HIV was the heterosexual route of transmission (94.53%), followed by unsafe sex with high-risk partners 6.16% and men who have sex with men (MSM) 3.01%. This can be explained by the mode of sexual activity practiced in the population. The study found that about 53.21% of HIV/AIDS patients on ART had one or more OIs compared to 46.79% who had no OI. This agrees with the prevalence of 48%, 46.7% and 58% documented by Mitiku et al, Sun et al and Balkhair et al, respectively.7-9 However, prevalence in the present study is higher than various studies conducted in Nigeria and Southern India, which documented 22.4%, 35.7% and 8.3% prevalence, respectively.10-12 This might be due to methodological differences in selecting study subjects. Moreover, South India’s literacy rate is comparatively higher as compared to Haryana’s; the present study found a significant association between education and OIs. This may explain the lower prevalence of OIs in the South. Also, it was lower as compared to the South Ethiopia study with a prevalence of 88.4%.13 This could be due to differences in availability and duration of HAART, the difference in CD4 level, clinical staging and the difference in host immunity of study subjects.
The present study revealed that TB (48.32% of total OIs) is the predominant OI identified, with a prevalence of 25.71% (188/731). Other studies done worldwide also had the same observation and TB was the most common OI found in PLHIV.7,13,14 TB enhances the progression of HIV infection by inducing immune activation. Candidiasis and herpes zoster were the second and the third most prevalent OIs in the present study, at 13.8% (101/731) and 7.25% (53/731), respectively. However, in many other studies, Candidiasis was found to be the most common OI as summarized in Table 4.7,9-13,15-20
|
Table 4. Comparison Between Different Studies Vis-a-Vis Present Study
|
|
Study
|
Prevalence of OIs
|
Most common OIs
|
|
Most common
|
2nd most common
|
3rd most common
|
|
Our study (2022)
|
53.21%
|
Tuberculosis (48.32%)
|
Candidiasis (25.7%)
|
Herpes zoster (13.6%)
|
|
International studies
Mitiku et al7 (2015)
Solomon et al13 (2018)
Balkhair et al9 (2012)
Iroezindu et al10 (2013)
Chanie et al (in children)17 (2021)
|
48%
88.4%
58%
22.4% (76/339)
5.53%
|
Tuberculosis (21.23%)
Tuberculosis (18%)
Pneumocystis jirovecii pneumonia (25%)
Candidiasis (8.6%)
Pneumonia (35.63%)
|
Herpes zoster (11.2%)
Community-acquired pneumonia (16.3%)
Cryptococcal meningitis (22%)
Tuberculosis (7.7%)
Tuberculosis (28.74%)
|
Oral candidiasis (9.5%)
Oral candidiasis (15.3%)
CMV retinitis (17%)
Dermatitis (5.6%)
Oral Candidiasis (10.34%)
|
|
Indian studies
Vinod et al15 (2018)
Ghate et al11 (2009)
Srirangaraj et al12 (2011)
Singh et al16 (2003)
Bariha et al18 (2018)
Saldanha et al19 (2008)
Sharma20 (2004)
|
23.5%
35.7%
8.3%
|
Candidiasis (52%)
Tuberculosis (15.4%)
Tuberculosis (53.4%)
Oral candidiasis (59%)
Tuberculosis (51%)
Tuberculosis (45.3%)
Tuberculosis (71%)
|
Tuberculosis (50%)
Oral Candidiasis (11.3%)
Oral Candidiasis (27.2%)
Tuberculosis (56%)
Oral Candidiasis (43%)
Candidiasis (34.5%)
Candidiasis (39.3%)
|
Herpes zoster (10.1%)
Herpes zoster (14.7%)
Cryptosporidiosis (47%)
Cryptosporidiosis (6.8%)
Cryptosporidiosis (17.5%)
Pneumocystis jirovecii pneumonia (7.4%)
|
In the present study, the prevalence of cryptococcal meningitis was 2.05%, significantly higher than in the study conducted by Mitiku, with a prevalence of 0.28%.7 This could be due to increasing diagnostic availability (radiological and serology) and high suspicion of disease. There were 63 co-infections of different OIs observed in the present study. Of these, 55 had 2 co-infections, 7 had 3 co-infections and 1 patient had 4 co-infections. Also, TB with candidiasis was the most common co-infection (32 cases), followed by TB with cryptosporidiosis (4 cases). This was similar to studies conducted in Eastern Ethiopia and Northwest Ethiopia.7,21
A higher proportion of TB and candidiasis co-infection in the present study may be explained by a higher prevalence of these two OIs among the study participants. Double and triple OIs have also been reported from studies in India and Nigeria.5,10 Prevalence of OIs among patients with comorbid viral hepatitis was comparable. No statistically significant association was observed (p = 0.053). This could be due to the small sample size of hepatitis B virus (HBV) and hepatitis C virus (HCV) reactive patients. However, the highest prevalence of OIs was depicted among hepatitis B surface antigen (HBsAg) reactive patients (n = 14/18, 77.78%).
The present study was conducted among HIV patients taking ART for 1 month or more. The prevalence of OIs was significantly higher in patients on ART for <4 months (83.33%), and the prevalence decreased in the subsequent months. This was similar to various previous studies and may be because HAART improves patient’s CD4 count and therefore the prevalence of OIs decreases overtime.22,23 HIV-associated OIs and other related infections continue to occur in HIV-positive patients, but since the introduction of HAART, most infections occur at rates that are substantially lower than those seen in the pre-HAART era.
WHO clinical stage IV and III showed highest prevalence while least prevalence was observed among clinical stage I patients. This was similar to study in Northwest Ethiopia.21 In WHO stages II, III and IV, there is marked reduction in CD4 count, which may be the reason for the increased prevalence of OIs as in our study. The prevalence of OIs was highest (n = 225/225, 100%) among HIV-infected patients with CD4 count <200/mm3. In contrast, the prevalence was significantly lower in patients with a CD4 count of >500/mm3, with a prevalence of only 5.41%. Other studies from India have also reported a high risk of developing OIs such as TB, Pneumocystis jirovecii pneumonia and cryptococcal meningitis among patients with CD4 counts <200 cells/mm3.23 This finding appears accurate since CD4 cells play a central role in the activation of humoral and cellular immune response in the fight against infection. Hence, low CD4 count increases susceptibility to OIs.21
In the present study, OI was significantly higher in patients with BMI (kg/m²) of <18.5 (underweight; 83.94%). BMI is an important indicator of nutritional status in patients with HIV infection. Emaciation is a common condition during the early period of HIV, and there is some evidence that higher BMI is associated with more robust CD4+ T-cell recovery in HAART-treated patients.24 Li et al demonstrated that HIV-infected patients with higher BMI at pre-treatment exhibit better immune reconstitution overtime after HAART initiation.25 Also, patients with body weight <52.72 ± 7.21 kg were more prone to develop OIs. This finding was similar to a study conducted by Inamdar et al.14
Opportunistic infections were significantly higher in patients with poor adherence to ART (99.12%). This was similar to the findings in the study conducted by Iroezindu et al.10 Fonsah et al conducted a study where subjects with CD4 cell counts <200 cells/µL had a lower proportion of good adherence than subjects with CD4 cell counts ≥200 cells /µL.26 Therefore, people with poor adherence have a low CD4 count that translates to an increased incidence of OIs. Poor adherence to ART also causes progression of HIV, decreased CD4 count and hence can result in more OIs as already discussed.
Significant association was seen between hemoglobin (g/dL) and patients with OI with mean ± SD of hemoglobin (g/dL) <9.87 ± 1.83 g/dL. This was similar to a study by Iroezindu et al.10 Srikantia et al demonstrated that both the cell-mediated immune response and bactericidal capacity of leukocytes in children with hemoglobin levels below 10 g/dL were significantly depressed.27
Significant association was seen between protein, albumin and OIs. Studies in the past decade have suggested that low albumin levels in HIV-infected patients are associated with rapid progression to AIDS and may account for increased mortality. Studies have suggested baseline albumin levels to be a good predictor of survival in patients with low CD4 count.28-30 This may be attributable to nutritional factors, enteropathy and acute phase reactant proteins. Hence, the National AIDS Control Organization (NACO) in India provides nutritional supplements to those HIV-infected cases inducted for ART and nutritional counseling for others as a part of a national policy.31 In developing countries where many people live below the poverty line, serum albumin would be a useful surrogate test for predicting the severity of HIV infection and the clinical monitoring of response to ART.
There were some limitations of the present study. As a cross-sectional study, cause-effect relationships cannot be assessed. Therefore, the data on the natural history pattern of disease and survival of hospitalized patients with HIV/AIDS could not be established. The study’s endpoint is restricted to the in-hospital period; hence, the full access to patient’s follow-up clinical data after being discharged was not always available.
The present study shows TB as the commonest OI in overall population of PLHIVs in Haryana followed by candidiasis and herpes zoster. Baseline CD4 cell count <200 cells/mm3, baseline WHO clinical stages III and IV and ART nonadherence were strongly associated with the prevalence of OIs. Lower income, education and socioeconomic status were also associated with a higher prevalence of OIs. Weight, BMI, albumin, hemoglobin level are strong predictors for the occurrence of OIs.
CONCLUSION
Presently, India has the third-largest population of HIV-infected individuals after South Africa and Nigeria. HIV patients are susceptible to a variety of OIs depending upon clinical status, WHO grading and CD4 count. It is noteworthy that OIs can have atypical presentations and multisystem involvement. Various factors like adherence to ART, socioeconomic and education status of patients can influence the occurrence and outcome of these deadly infections. Hence, there is a need for surveillance and a high degree of suspicion of these infections in HIV patients to ensure early diagnosis and intervention. Moreover, interventions need to be designed to promote easy and early access to HIV testing and early enrollment of HIV-infected individuals into ART services seeing that the use of ART was found to reduce the prevalence of OIs by 4th month. Individuals who continue to have low CD4 cell counts while on ART should be aggressively evaluated for OIs and practical efforts to optimize their immunological recovery should be made.
Conflict of Interest: Nil.
External Funding Support: Nil.
REFERENCES
- Kaplan JE, Masur H, Holmes KK, Wilfert CM, Sperling R, Baker SA, et al. USPHS/IDSA guidelines for the prevention of opportunistic infections in persons infected with human immunodeficiency virus: an overview. USPHS/IDSA Prevention of Opportunistic Infections Working Group. Clin Infect Dis. 1995;21 Suppl 1:S12-31.
- Bacchetti P, Moss AR. Incubation period of AIDS in San Francisco. Nature. 1989;338(6212):251-3.
- Alcabes P, Muñoz A, Vlahov D, Friedland GH. Incubation period of human immunodeficiency virus. Epidemiol Rev. 1993;15(2):303-18.
- Bacchetti P, Osmond D, Chaisson RE, Oritz S, Rutherford GW, Swig L, et al. Survival patterns of the first 500 patients with AIDS in San Francisco. J Infect Dis. 1988;157(5):1044-7.
- Saha K, Firdaus R, Santra P, Pal J, Roy A, Bhattacharya MK, et al. Recent pattern of co-infection amongst HIV seropositive individuals in tertiary care hospital, Kolkata. Virol J. 2011;8:116.
- Mannheimer SB, Mukherjee R, Hirschhorn LR, Dougherty J, Celano SA, Ciccarone D, et al. The CASE adherence index: a novel method for measuring adherence to antiretroviral therapy. AIDS Care. 2006;18(7):853-61.
- Mitiku H, Weldegebreal F, Teklemariam Z. Magnitude of opportunistic infections and associated factors in HIV-infected adults on antiretroviral therapy in eastern Ethiopia. HIV AIDS (Auckl). 2015;7:137-44.
- Sun HY, Chen MY, Hsieh SM, Sheng WH, Chang SY, Hsiao CF, et al. Changes in the clinical spectrum of opportunistic illnesses in persons with HIV infection in Taiwan in the era of highly active antiretroviral therapy. Jpn J Infect Dis. 2006;59(5):311-6.
- Balkhair AA, Al-Muharrmi ZK, Ganguly S, Al-Jabri AA. Spectrum of AIDS defining opportunistic infections in a series of 77 hospitalised HIV-infected Omani patients. Sultan Qaboos Univ Med J. 2012;12(4):442-8.
- Iroezindu MO, Ofondu EO, Hausler H, van Wyk B. Prevalence and risk factors for opportunistic infections in HIV patients receiving antiretroviral therapy in a resource-limited setting in Nigeria. J AIDS Clinic Res. 2013;S3:002.
- Ghate M, Deshpande S, Tripathy S, Nene M, Gedam P, Godbole S, et al. Incidence of common opportunistic infections in HIV-infected individuals in Pune, India: analysis by stages of immunosuppression represented by CD4 counts. Int J Infect Dis. 2009;13(1):e1-8.
- Srirangaraj S, Venkatesha D. Opportunistic infections in relation to antiretroviral status among AIDS patients from south India. Indian J Med Microbiol. 2011;29(4):395-400.
- Solomon FB, Angore BN, Koyra HC, Tufa EG, Berheto TM, Admasu M. Spectrum of opportunistic infections and associated factors among people living with HIV/AIDS in the era of highly active anti-retroviral treatment in Dawro Zone hospital: a retrospective study. BMC Res Notes. 2018;11(1):604.
- Inamdar SA, Kosambiya JK, Modi A, Gohil A, Mehta A, Patel T. Age and opportunistic infections: prevalence and predictors among older people living with HIV. Natl J Community Med. 2018;9(8):610-3.
- Vinod PK, Radhakrishnan C, Pk S. Incidence and spectrum of opportunistic infections among HIV Infected patients attending Government Medical College, Kozhikode. J Assoc Physicians India. 2018;66(7):33-6.
- Singh A, Bairy I, Shivananda PG. Spectrum of opportunistic infections in AIDS cases. Indian J Med Sci. 2003;57(1):16-21.
- Chanie ES, Bayih WA, Birhan BM, Belay DM, Asmare G, Tiruneh T, et al. Incidence of advanced opportunistic infection and its predictors among HIV infected children at Debre Tabor Referral Hospital and University of Gondar Compressive specialized hospitals, Northwest Ethiopia, 2020: a multicenter retrospective follow-up study. Heliyon. 2021;7(4):e06745.
- Bariha PK, Mohapatra MK, Kullu BK, Karua PC, Biswal SB, Thakur A. Prospective study of opportunistic infections among HIV infected patients in VSS Institute of Medical Science and Research, Burla, Sambalpur, Odisha, India. Int J Adv Med. 2018;5(3):566-72.
- Saldanha D, Gupta N, Shenoy S, Saralaya V. Prevalence of opportunistic infections in AIDS patients in Mangalore, Karnataka. Trop Doct. 2008;38(3):172-3.
- Sharma SK, Kadhiravan T, Banga A, Goyal T, Bhatia I, Saha PK. Spectrum of clinical disease in a series of 135 hospitalised HIV-infected patients from north India. BMC Infect Dis. 2004;4:52.
- Damtie D, Yismaw G, Woldeyohannes D, Anagaw B. Common opportunistic infections and their CD4 cell correlates among HIV-infected patients attending at antiretroviral therapy clinic of Gondar University Hospital, Northwest Ethiopia. BMC Res Notes. 2013;6(1):534.
- Sun HY, Chen MY, Hsieh SM, Sheng WH, Chang SY, Hsiao CF, et al. Changes in the clinical spectrum of opportunistic illnesses in persons with HIV infection in Taiwan in the era of highly active antiretroviral therapy. Jpn J Infect Dis. 2006;59(5):311-6.
- Chakraborty N, Mukherjee A, Santra S, Sarkar RN, Banerjee D, Guha SK, et al. Current trends of opportunistic infections among HIV-seropositive patients from Eastern India. Jpn J Infect Dis. 2008;61(1):49-53.
- Koethe JR, Jenkins CA, Lau B, Shepherd BE, Wester W, Rebeiro PF, et al; North American AIDS Cohort Collaboration on Research and Design (NA-ACCORD). Higher time-updated body mass index: association with improved CD4+ cell recovery on HIV treatment. J Acquir Immune Defic Syndr. 2016;73(2):197-204.
- Li X, Ding H, Geng W, Liu J, Jiang Y, Xu J, et al. Predictive effects of body mass index on immune reconstitution among HIV-infected HAART users in China. BMC Infect Dis. 2019;19(1):373.
- Fonsah JY, Njamnshi AK, Kouanfack C, Qiu F, Njamnshi DM, Tagny CT, et al. Adherence to antiretroviral therapy (ART) in Yaoundé-Cameroon: association with opportunistic infections, depression, ART regimen and side effects. PLoS One. 2017;12(1):e0170893.
- Srikantia SG, Prasad JS, Bhaskaram C, Krishnamachari KA. Anaemia and immune response. Lancet. 1976;1(7973):1307-9.
- Sudfeld CR, Isanaka S, Aboud S, Mugusi FM, Wang M, Chalamilla GE, et al. Association of serum albumin concentration with mortality, morbidity, CD4 T-cell reconstitution among Tanzanians initiating antiretroviral therapy. J Infect Dis. 2013;207(9):1370-8.
- Olawumi HO, Olatunji PO. The value of serum albumin in pre-treatment assessment and monitoring of therapy in HIV/AIDS patients. HIV Med. 2006;7(6):351-5.
- Rankin WW, Brennan S, Schell E, Laviwa J, Rankin SH. The stigma of being HIV-positive in Africa. PLoS Med. 2005;2(8):e247.
- Ramakrishnan K, Shenbagarathai R, Kavitha K, Uma A, Balasubramaniam R, Thirumalaikolundusubramanian P. Serum zinc and albumin levels in pulmonary tuberculosis patients with and without HIV. Jpn J Infect Dis. 2008;61(3):202-4.