Abstract
Ivabradine has been used for over a decade in managing chronic coronary syndromes and heart failure (HF) with reduced ejection fraction (HFrEF). HF with preserved ejection fraction (HFpEF) accounts for 50% of the total HF cases carrying equal mortality and morbidity risk as HFrEF. Increased heart rate (HR) in such cases has been shown to be associated with poor clinical outcomes. Clinical conditions like inappropriate sinus tachycardia (IST) manifest with elevated HR without any specific triggers. Beta-blockers have been the preferred treatment of choice for both HFpEF and IST but are often ineffective or present with side effects due to their negative ionotropic effects. Ivabradine, through its inhibitory action on funny current (Ifc), reduces HR without altering the inotropic mechanism. Few case reports and small case series have documented its extended use and efficacy in reducing HR in these cardiac conditions. In this article, we present two cases who needed HR control, one with HFpEF and another case of IST syndrome. Ivabradine was successfully used in both these cases to control the elevated HR.
Keywords: Ivabradine, HFpEF, inappropriate sinus tachycardia
Ivabradine is a selective inhibitor of funny channel (Ifc), which are located in the sinoatrial node and are responsible for controlling the diastolic depolarization termed as If current and its activity can vary by the sympathetic and parasympathetic stimuli. Ivabradine, through a concentration-dependent mechanism, selectively inhibits the If channels and reduces the heart rate (HR) without altering the blood pressure (BP) or contraction or relaxation activity of the myocardium.1 It is a novel antiarrhythmic drug approved for the treatment of select heart failure (HF) patients.2
It was initially used as an antianginal drug and was later approved for use in HF with reduced ejection fraction (HFrEF) cases (EF <35%). The European Society of Cardiology (ESC) has recommended its application for reducing the risk of hospitalizations due to HF and cardiovascular death in New York Heart Association (NYHA) Class II-IV with left ventricular ejection fraction (LVEF) of ≤35% despite maximally tolerated doses of beta-blocker (BB). Nearly 50% of cases of HF patients have preserved EF (HFpEF) and bear similar mortality and morbidity outcomes as HFrEF.3
Increased HR in patients with HF is associated with poor outcomes. Patients with HFpEF have impaired left ventricular (LV) relaxation and increased HR during exercise, reducing the LV filling, which increases the LV filling pressure and causes reduced exercise tolerance. Since ivabradine reduces HR without causing any effect on BP, it has been used in specific cases for managing HR when BB or calcium channel blockers (CCBs) are contraindicated.4
Ivabradine has established itself as an HR-modulating agent with its prime role in chronic coronary syndromes and HFrEF. It has also been recognized for its extended use in other unapproved conditions like inappropriate sinus tachycardia (IST) and cases of HFpEF.
The two cases presented here are examples of extended use of ivabradine in HFpEF and IST. Off-label indications are fully justified when necessary, as the side effects are rare and not serious.
CASE REPORTS
Case 1
A 63-year-old female presented with history of Class IV dyspnea, cough, wheezing, pedal edema and extreme fatigue in June 2022. She was normotensive and nondiabetic with a history of chronic obstructive pulmonary disease (COPD). She was on oral bronchodilators, nebulizers and continuous positive airway pressure (CPAP) at night on the advice of a pulmonologist. She was on thyroid supplements and was euthyroid at presentation. Past medical history revealed repeated admissions in the last 13 years for episodic bronchospasm, worsening dyspnea and HF.
On examination, the patient had sinus tachycardia (HR 130/min), BP was 96/70 mmHg, jugular venous pressure (JVP) was elevated; pedal edema was noted. Cardiovascular examination revealed right ventricular (RV) heave, loud pulmonic closure sound (P2), Grade 2/6 ejection systolic murmur at the left sternal border and pansystolic tricuspid regurgitation murmur was heard. Routine blood tests were normal, thyroid-stimulating hormone (TSH) was normal and there was a 10-fold increase in N-terminal pro-brain natriuretic peptide (NT-proBNP) levels.
An electrocardiogram (ECG) showed sinus rhythm, HR 133/min, right axis deviation and RV hypertrophy with strain (Fig. 1A). X-ray chest showed cardiomegaly, a prominent pulmonary artery segment and evidence of pulmonary hypertension. Lung fields showed peribronchiolar haze. The echocardiogram revealed normal LV size, no regional wall motion abnormalities (RWMA) and an LVEF of 62%. There was evidence of severe pulmonary arterial hypertension (PAH) with RV dysfunction. She was diagnosed with COPD, severe PAH with RV dysfunction, preserved LV systolic function (HFpEF) and right-sided HF.
The patient was started on digoxin, diuretics and pulmonary vasodilators (tadalafil), oral bronchodilators, as well as nebulizers, antibiotics and bilevel-positive airway pressure (BiPAP). On day 3, she developed persistent sinus tachycardia; hence, ivabradine 5 mg twice daily was added as BB were contraindicated due to COPD. Three days later, ECG revealed a sinus rhythm rate of 82/min (Fig. 1B).
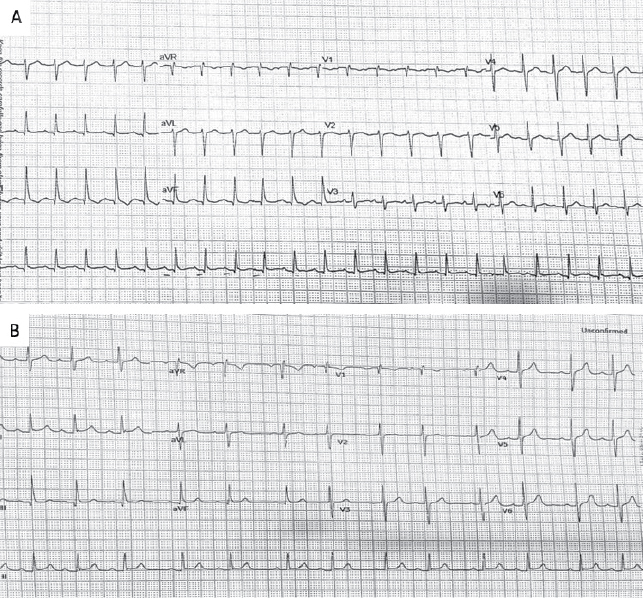
Figure 1. ECG at admission showing sinus rhythm, 133/min, right axis deviation (A). ECG 3 days after starting ivabradine showing sinus rhythm, 82/min (B).
Case 2
A 70-year-old female, NRI, from USA, came for a routine annual review in September 2022. She had a history of intermittent episodic palpitations with sweating for a short duration for the past 5 years. There were 3 episodes of presyncope, mainly on effort and emotion associated with severe palpitations. She was a known case of mild hypertension for 20 years and had a history of intermittent bronchospasm requiring bronchodilator inhalers.
She had undergone a complete cardiac evaluation in USA. Her ECG showed a left bundle branch block (LBBB). Biochemical parameters including thyroid profile were normal. Echocardiogram did not show any RWMA and LVEF was normal. A treadmill test (TMT) showed normal effort tolerance with no symptoms or evidence of arrhythmias except sinus tachycardia and LBBB. In August 2019, she underwent 14 days of patch monitoring, which revealed sinus rhythm, rate 61-126/min and occasional supraventricular ectopics. There were no ventricular arrhythmias or pauses. During episodes of symptomatic palpitations, monitoring revealed sinus tachycardia, which lasted for 10 to 15 minutes.
She was diagnosed with symptomatic IST syndrome. The patient was started on oral ivabradine 5 mg twice daily, spironolactone for hypertension and bronchodilator inhalers whenever needed. She came for an annual review in September 2022 and expressed 90% symptomatic improvement with medication. Her pulse rate was 76/min, regular and her BP was 130/70 mmHg.
The cardiovascular and chest examinations were normal. ECG revealed sinus rhythm, 76/min and LBBB. Her echocardiogram was normal; 640 slice computerized tomography (CT) coronary angiogram revealed evidence of insignificant CAD. She was reassured and continued on ivabradine and was advised to come for a follow-up every 6 months or earlier, if warranted, by symptoms.
DISCUSSION
In HF, there is an increase in HR as a response to the reduced cardiac output. But this elevated HR leads to increased oxygen demand by the myocardium resulting in the worsening of hemodynamic mechanism resulting in ventricular dysfunction and poor clinical outcomes. Patients with HFpEF have impaired LV relaxation and increased HR during exercise, reducing the LV filling, which in turn increases the LV filling pressures and decreases exercise tolerance. Drugs like BBs have not shown any reduction in mortality due to cardiovascular causes in HFpEF.4 Due to their negative ionotropic effect, no improvement was observed in exercise tolerance or peak oxygen uptake.5 Ivabradine has shown promising results as it reduces HR by selectively acting only on the If channels.6
Ivabradine exerts a negative chronotropic effect by reducing the spontaneous phase IV depolarization in the sinoatrial node by blocking the If channels, which causes an increase in the diastolic time.6 Data from a study by Kosmala et al comparing ivabradine and placebo in 61 patients with HFpEF for 7 days has shown significant improvement in exercise capacity in the former group (metabolic equivalents [METs] was 1.5 ± 1.2 vs. 0.4 ± 1.2; p = 0.001) along with improvement in peak VO2 (3 ± 3.6 mL/kg/min vs. 04 ± 2.7 mL/kg/min; p = 0.003).7 Another study by Pal et al has shown significant improvement in VO2 (p = 0.003) and reduced submaximal exercise capacity with dose titration.8
Ivabradine has been routinely used to control HR in cases of HFrEF, angina and chronic coronary syndromes. In the present cases, BBs were contraindicated because of bronchospasm. For controlling the HR, non-dihydropyridine CCBs like verapamil were found ineffective owing to the risk of reduction in systemic arterial pressure, negative ionotropic effect and negative impact on gas exchange.
IST is a rare form of atrial tachycardia due to improper rapid depolarization in the sinus node. Clinically, the resting HR is usually high (90-100 beats/min), which would increase abnormally on physical activity. It manifests with symptoms of presyncope, syncope, dizziness, weakness, palpitation and exercise intolerance. Management chiefly includes BBs, CCBs or antiarrhythmic drugs. But in nearly one-third cases, these drugs fail to relieve the symptoms and are associated with side effects. Ivabradine, due to its role in controlling HR, has shown promising results as its extended indication in IST.9
The correction of the IST occurs without measurable bradycardia since ivabradine acts as an open channel blocker. Even when used in combination with BB, it is safe and reduces the risk of hypotension that occurs with BB since the dosage of BB is less in combination therapy. Data from a large case series in patients affected with IST have shown a mean HR reduction of 22 beats/min at 3 months and 34 beats/min after 6 months with ivabradine.10
Even the quality of life score, short-form 36 items (SF-36) showed significant improvement (p = 0.001) and was well-tolerated.11 Even in renal transplant cases with IST, where BB was not helpful and CCB were contraindicated due to drug interactions with immunosuppressants, ivabradine was noted to be effective in controlling HR.12 The ESC guidelines have recommended BBs as first-line therapy for IST. Ivabradine, alone or with BBs, can be considered in symptomatic patients with IST as a Class IIa recommendation.13
Other drugs, like nondihydropyridine CCBs such as verapamil, diltiazem and catheter ablation for refractory cases, are no longer recommended for IST.
Ivabradine has been approved as a second-line drug for chronic stable angina in BB intolerant patients or in whom BBs are contraindicated. Ivabradine, though an off-label indication, can be considered to control HR in HFpEF and IST in clinical practice as there are no adverse effects in these cases.14
CONCLUSIONS
In patients with HFpEF and IST, lowering HR is beneficial to reduce myocardial oxygen requirement and cardioprotection. Selective action of lowering HR without altering the BP shows promising results for ivabradine in such cases. It also improves exercise capacity and improves the quality of life.
Ivabradine has been proven to be effective for HFrEF and angina, but it has also shown potential benefit in HFpEF and IST. With the increased use of ivabradine in off-label indications, we hope additional clinical studies will be conducted for consideration in future guidelines.
Conflict of Interest: The authors have no conflicts of interest to declare.
Financial Disclosure: None.
REFERENCES
- Deedwania P. Selective and specific inhibition of If with ivabradine for the treatment of coronary artery disease or heart failure. Drugs. 2013;73(14):1569-86.
- Koruth JS, Lala A, Pinney S, Reddy VY, Dukkipati SR. The clinical use of ivabradine. J Am Coll Cardiol. 2017;70(14):1777-84.
- Komajda M, Isnard R, Cohen-Solal A, Metra M, Pieske B, Ponikowski P, et al. Effect of ivabradine in patients with heart failure with preserved ejection fraction: the EDIFY randomized placebo-controlled trial. Eur J Heart Fail. 2017;19(11):1495-503.
- Yamamoto K. β-blocker therapy in heart failure with preserved ejection fraction: importance of dose and duration. J Cardiol. 2015;66(3):189-94.
- Conraads VM, Metra M, Kamp O, De Keulenaer GW, Pieske B, Zamorano J, et al. Effects of the long-term administration of nebivolol on the clinical symptoms, exercise capacity, and left ventricular function of patients with diastolic dysfunction: results of the ELANDD study. Eur J Heart Fail. 2012;14(2):219-25.
- DiFrancesco D, Camm JA. Heart rate lowering by specific and selective I(f) current inhibition with ivabradine: a new therapeutic perspective in cardiovascular disease. Drugs. 2004;64(16):1757-65.
- Kosmala W, Holland DJ, Rojek A, Wright L, Przewlocka-Kosmala M, Marwick TH. Effect of If-channel inhibition on hemodynamic status and exercise tolerance in heart with preserved ejection fraction: a randomized trial. J Am Coll Cardiol. 2013;62(15):1330-8.
- Pal N, Sivaswamy N, Mahmod M, Yavari A, Rudd A, Singh S, et al. Response to letter regarding article, “the effect of selective heart rate slowing in heart failure with preserved ejection fraction”. Circulation. 2016;133(16):e604.
- Khan S, Hamid S, Rinaldi C. Treatment of inappropriate sinus tachycardia with ivabradine in a patient with postural orthostatic tachycardia syndrome and a dual chamber pacemaker. Pacing Clin Electrophysiol. 2009;32(1):131-3.
- Calo L, Rebecchi M, Sette A, Martino A, de Ruvo E, Sciarra L, et al. Efficacy of ivabradine administration in patients affected by inappropriate sinus tachycardia. Heart Rhythm. 2010;7(9):1318-23.
- Benezet-Mazuecos J, Rubio JM, Farre J, Quinones MA, Sanchez-Borque P, Macia E. Long-term outcomes of ivabradine in inappropriate sinus tachycardia patients: appropriate efficacy or inappropriate patients. Pacing Clin Electrophysiol. 2013;36(7):830-6.
- Goyal VK, Godara S, Sadasukhi TC, Gupta HL. Management of inappropriate sinus tachycardia with ivabradine in a renal transplant recipient. Drug Discov Ther. 2014;8(3):132-3.
- Brugada J, Katritsis DG, Arbelo E, Arribas F, Bax JJ, Blomström-Lundqvist C, et al; ESC Scientific Document Group. 2019 ESC Guidelines for the management of patients with supraventricular tachycardia: the Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC): Developed in collaboration with the Association for European Paediatric and Congenital Cardiology (AEPC). Eur Heart J. 2020;41(5):655-720.
- Othman KMS, Mostafa MAR, Yosef AE, Abdeltawab AA. Safety and efficacy of off-label use of ivabradine in patients with acute heart failure. J Saudi Heart Assoc. 2019;31(4):179-87.