Abstract
Scrub typhus is an acute febrile illness caused by Orientia tsutsugamushi, a Gram-negative intracellular organism transmitted by Leptotrombidium mites, with wild rats serving as natural reservoirs. The disease is more common in the Tsutsugamushi Triangle, often afflicting travelers and creating diagnostic challenges in clinical practice. We present the case of a diabetic patient who acquired the infection while visiting an agricultural farm. Our discussion covers clinical manifestations, diagnostic markers and treatment modalities, emphasizing the significance of early recognition and the benefits of prompt treatment. The importance of searching for an eschar, a key physical sign, is underscored and potential serious outcomes are discussed. Recent advances and preventive measures are also highlighted. This synthesis of research and clinical insights aims to enhance global awareness, prompt diagnosis and effective management of scrub typhus.
Keywords: Eschar, fever-mite, tsutsugamushi, scrub typhus, international travelers
Scrub typhus is an acute febrile illness caused by infection with Orientia tsutsugamushi, an intracellular obligate Gram-negative organism. It is transmitted to humans by the bite of the infected chigger, the mite of Leptotrombidium. Wild rats serve as the natural reservoir, with humans as accidental victims. Chiggers, measuring 0.2 mm, are challenging to visualize with the naked eye. They typically inhabit scrubs, the transitional area between woods and clearings, hence the term “Scrub Typhus”. In tropical regions, infections can occur year-round, while in the Far East, infections peak from July to September.1
The geographical distribution of this disease forms a triangular area extending from northern Japan in the east to eastern Russia in the north, Afghanistan and Pakistan in the west and northern Australia in the south, known as the Tsutsugamushi Triangle. Approximately half of the human population resides in this area. Scrub typhus is often acquired during occupational or agricultural exposure.2 An estimated 1 million cases occur annually and around 1 billion people in the endemic areas are possibly being infected at some point. In India, although clear statistics are lacking, a literature search from the past 10 years reported 18,781 confirmed cases.3
The incubation period ranges from 6 to 20 days, with an average of 10 days. Patients commonly present with high fever, cough, malaise, anorexia, ocular pain, lymphadenopathy and splenomegaly. Severe cases may involve pneumonitis, encephalitis, myocarditis, hepatitis, renal failure and, rarely, complications such as acute respiratory distress syndrome, circulatory failure and disseminated intravascular coagulation. A diagnostic sign is the presence of an eschar at the chigger bite site, with a maculopapular rash potentially developing on the 5th to 8th day. Mortality rates vary from 1% to 60%, depending on the strain and geographical area, with poor prognostic factors including age over 60, high initial leukocyte count, elevated C-reactive protein (CRP), abnormal liver function tests and the absence of an eschar.4
Doxycycline is the preferred treatment, and alternatives include azithromycin, rifampin and chloromycetin. Chemoprophylaxis with weekly doxycycline starting a week before and continuing for 6 weeks after exposure is advisable. Wearing appropriate clothing or using repellent to prevent mite bites and employing a cloth barrier while in the scrubs are recommended preventive measures.5
CASE SUMMARY
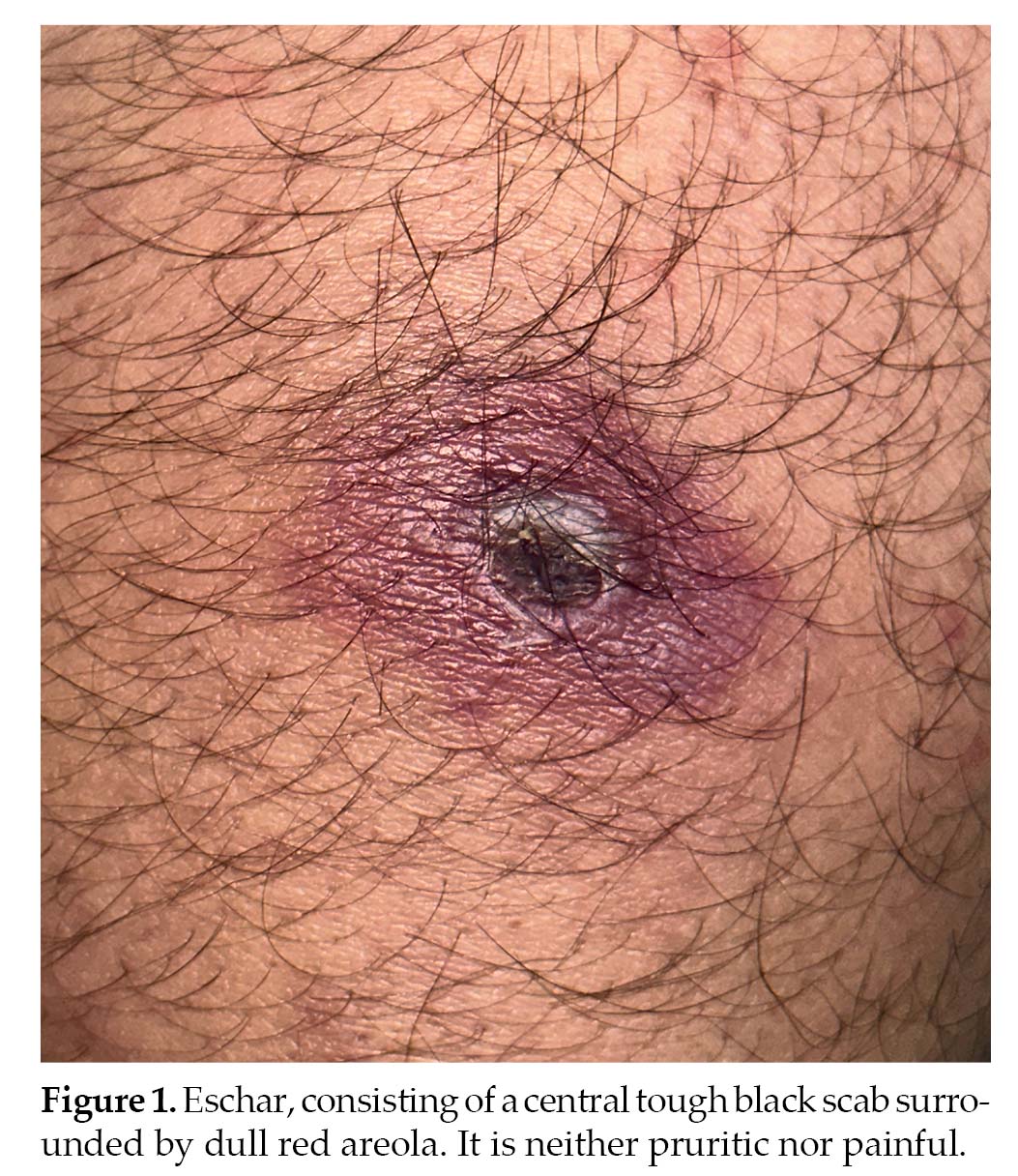
A 54-year-old male was admitted to the hospital on 24th July, 2023 with an 8-day history of fever with chills. He had an ulcer with surrounding erythema on the left thigh (Fig. 1), and vaguely recalled being bitten by an insect in the same area a week before the ulcer developed. This incident occurred during an outdoor party at a friend’s farmhouse in a suburban area. The patient developed an erythematous maculopapular rash on the day of admission (Fig. 2). He had a 20-year
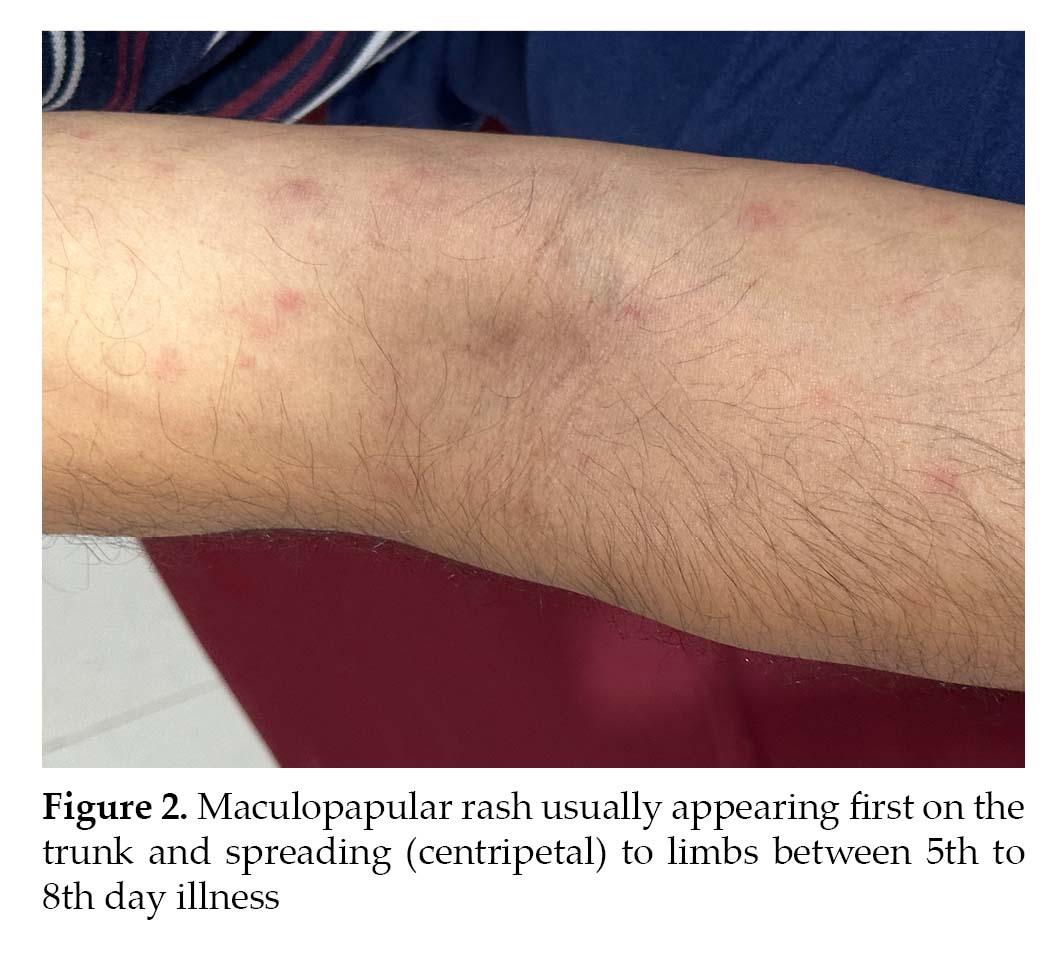
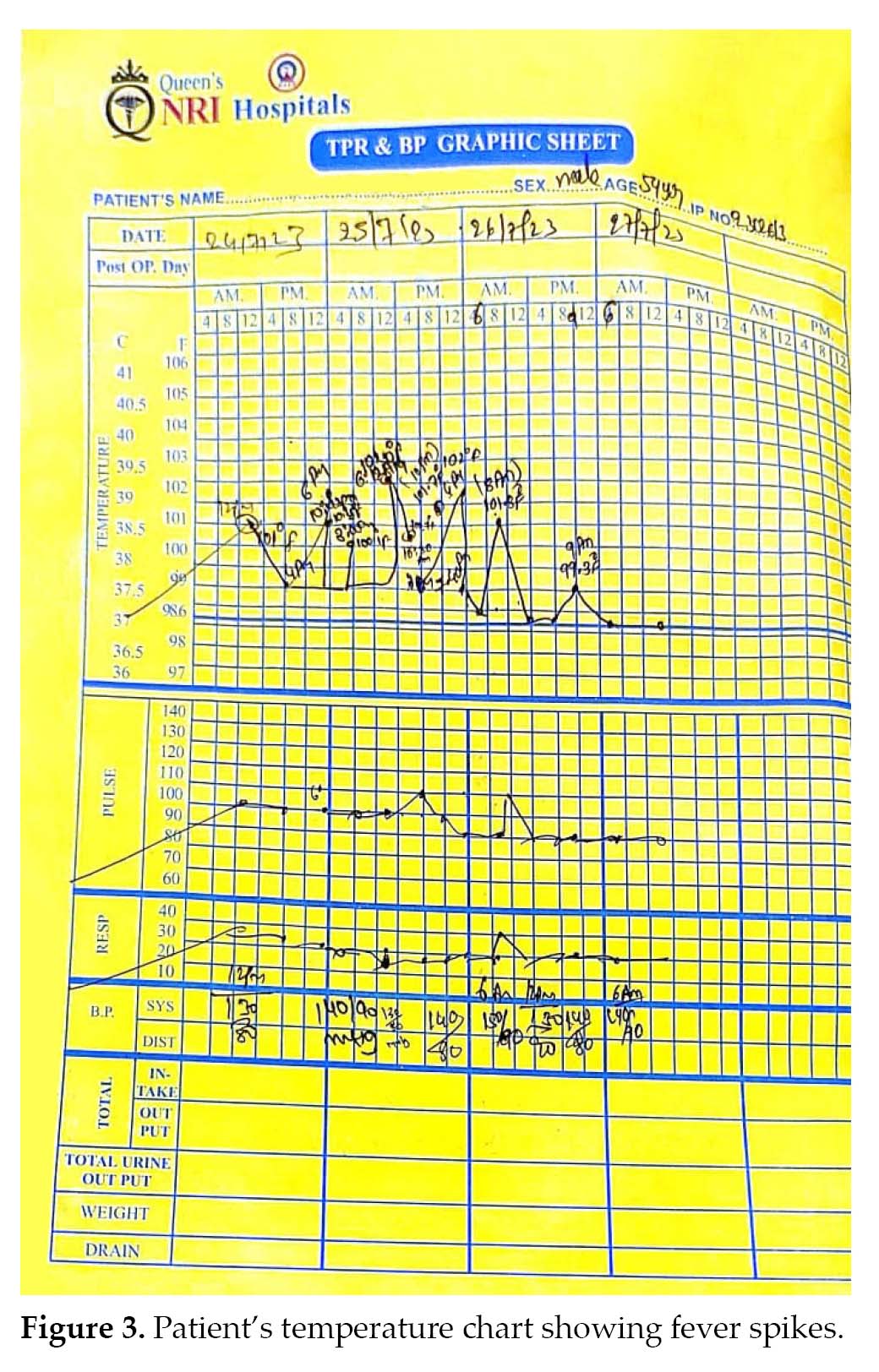
history of diabetes treated with a combination of insulin aspart and insulin aspart protamine and had taken an antibiotic (amoxicillin clavulanate) initially but discontinued it due to gastrointestinal side effects. He had taken cefuroxime for 3 days before admission. The patient was febrile with a temperature of 103°F (Fig. 3), normal blood pressure and a pulse rate of 101/min. Physical examination revealed clear lungs, tachycardia, mild abdominal distension with no tenderness and restlessness. Laboratory investigations are detailed in Table 1.
Based on clinical presentation, the presence of an eschar and a positive rapid immunochromatographic test for IgM against O. tsutsugamushi, a diagnosis of scrub typhus was established. The patient was treated with doxycycline and azithromycin and showed a favorable response by the 3rd day, with the fever resolving and ulcer healing by the 5th day. The patient was discharged on a regimen of doxycycline and azithromycin, and after a 10-day follow-up, the patient was healthy with complete healing of the ulcer.6
|
Table 1. Laboratory Investigations
|
|
TWBC: 7,000/µL
Hb%:14.0 g
CRP: 23.71 mg
Peripheral smear: Normal
LDH: 364 Unit/L
Urine microscopy: 6-8 pus cells
Dengue serology: Negative
QBC malaria: Negative
IgM typhoid: Negative
HBsAg: Negative
HCV: Negative
HIV: Negative
IgM scrub typhus: Positive
Ultrasound abdomen: Cholelithiasis
Chest X-ray: Normal
ECG: Normal
Urine culture and sensitivity: No growth
Blood culture and sensitivity: No growth
|
TWBC = Total white blood cells; Hb = Hemoglobin; CRP = C-reactive protein; LDH = Lactate dehydrogenase; QBC = Quantitative buffy coat; IgM = Immunoglobulin M; HbsAg = Hepatitis B surface antigen; HCV = Hepatitis C virus; HIV = Human immunodeficiency virus; ECG: Electrocardiogram.
DISCUSSION
The patient likely contracted scrub typhus while visiting an agricultural farm, commonly associated with activities in scrubs or agriculture. The presence of a typical eschar at the insect bite site supported the diagnosis, although its absence does not exclude the disease. The patient exhibited high-grade spiky fever, a common symptom in scrub typhus cases. The maculopapular rash on the 8th day aligned with the typical presentation, and although the patient had a normal leukocyte count, literature suggests initial lymphopenia followed by lymphocytosis is common. Poor prognostic indicators, such as increased CRP, were present in this case. A positive rapid test for IgM is a common method for diagnosing scrub typhus in developing countries. Pulmonary involvement, often seen as patchy pneumonia, did not manifest radiologically in this patient.7
Differential diagnoses include leptospirosis, dengue, malaria, typhoid, anthrax, rickettsial pox, tularemia and viral fevers with thrombocytopenia. Diagnosis may be challenging in the absence of a typical eschar.
Interestingly, in human immunodeficiency virus (HIV)-
positive patients infected with certain strains of scrub typhus, a dramatic decrease in viral load has been observed, sparking research interest.8 Treatment choices involve doxycycline and azithromycin, either individually or in combination, depending on the clinical scenario. Our patient responded favorably to treatment, emphasizing the importance of timely intervention. If a patient does not respond, re-evaluation of the diagnosis or consideration of drug resistance is crucial.9
CONCLUSION
Scrub typhus can be fatal if not diagnosed early and treated appropriately. Clinical presentations and laboratory parameters may mimic other febrile illnesses, necessitating a thorough search for an eschar as a vital diagnostic clue. Scrub typhus should be considered in the differential diagnosis, particularly when treating febrile illnesses in travelers from endemic areas.
Acknowledgment
We sincerely thank Dr Chalasani Vijayalakshmi, Chairperson of the Queen’s NRI Hospital, Visakhapatnam, for allowing us to publish the case.
Declarations
Funding: None.
Conflict of interest: None declared.
Ethical approval: Not required.
REFERENCES
- Ogawa M, Hagiwara T, Kishimoto T, Shiga S, Yoshida Y, Furuya Y, et al. Scrub typhus in Japan: epidemiology and clinical features of cases reported in 1998. Am J Trop Med Hyg. 2002;67(2):162-5.
- Sharma PK, Ramakrishnan R, Hutin YJ, Barui AK, Manickam P, Kakkar M, et al. Scrub typhus in Darjeeling, India: opportunities for simple, practical prevention measures. Trans R Soc Trop Med Hyg. 2009;103(11):1153-8.
- Devasagayam E, Dayanand D, Kundu D, Kamath MS, Kirubakaran R, Varghese GM. The burden of scrub typhus in India: a systematic review. PLoS Negl Trop Dis. 2021;15(7):e0009619.
- Kim DM, Kim SW, Choi SH, Yun NR. Clinical and laboratory findings associated with severe scrub typhus. BMC Infect Dis. 2010;10:108.
- Olson JG, Bourgeois AL, Fang RC, Coolbaugh JC, Dennis DT. Prevention of scrub typhus. Prophylactic administration of doxycycline in a randomized double blind trial. Am J Trop Med Hyg. 1980;29(5):989-97.
- Rodkvamtook W, Prasartvit A, Jatisatienr C, Jatisatienr A, Gaywee J, Eamsobhana P. Efficacy of plant essential oils for the repellents against chiggers (Leptotrombidium imphalum) vector of scrub typhus. J Med Assoc Thai. 2012;95 Suppl 5:
S103-6.
- Chen HC, Chang HC, Chang YC, Liu SF, Su MC, Huang KT, et al. Chest radiographic presentation in patients with scrub typhus. Trans R Soc Trop Med Hyg. 2012;106(1):48-53.
- Watt G, Kantipong P, de Souza M, Chanbancherd P, Jongsakul K, Ruangweerayud R, et al. HIV-1 suppression during acute scrub-typhus infection. Lancet. 2000;356(9228):475-9.
- Varghese GM, Dayanand D, Gunasekaran K, Kundu D, Wyawahare M, Sharma N,etal; INTREST Trial Investigators. Intravenous doxycycline, azithromycin, or both for severe scrub typhus. N Engl J Med. 2023;388(9):792-803.