Abstract
Objective: The present study was carried out to evaluate the impact of Pharmacovigilance Programme of India (PvPI) initiative to reduce the use of sodium valproate/valproic acid (SV/VA) in the women of childbearing age group. Methods: In our questionnaire-based study, 251 health care professionals (HCPs) participated from 41 medical colleges across India, which are also working as Adverse drug reaction Monitoring Centres (AMCs) under PvPI. Results: The data collected at the National Coordination Centre (NCC) shows the significant decrease in the use of SV/VA in the women of childbearing age group after the PvPI initiative on Information, Education, and Communication (IEC) materials for HCPs. However, it was found that 40% of HCPs of Gynecology and Neurology Department were still not aware of the initiative taken by the Government of India to reduce the use of SV/VA in the women of childbearing age group. Conclusion: PvPI, therefore, needs to take more measures to increase the reach of their resource materials to all HCPs.
Keywords: Sodium valproate, valproic acid, pharmacovigilance, AMCs, health care professionals
Sodium valproate (SV) is chemically sodium 2-propylpentanoate. It is also known as sodium dipropylacetic acid, sodium 2-propylvalerate, sodium dipropylacetate, sodium di-n-propylacetate, etc. SV is a white crystalline powder with a characteristic odor of valproic acid (VA). The chemical name of VA is 2-propylpentanoic acid. It is also known as n-dipropylacetic acid, 2-propylvaleric acid, dipropylacetic acid. Valproic acid is a colorless viscous liquid1.
Global Status of SV
In 1981, the Central Drugs Standard Control Organisation (CDSCO) approved an application of SV/VA for the treatment of all forms of epilepsy in India by the manufacturer. SV freeze dried powder 400 mg/mL injection was approved in year 1999 for the treatment of generalized epilepsy as well as for partial epilepsy in patients for whom oral therapy is temporarily not possible. SV tablet/syrup was approved in year 2000 for additional indications of manic episodes associated with bipolar disorders2.
Currently, it is available in different strength. Divalproex tablets 125 mg, 250 mg, 500 mg, 750 mg, and 1 g; syrup - 250 mg/5 mL. Valproic acid tablet - 200 mg, 300 mg, 500 mg; injection (sodium valproate) 100 mg/mL and 250 mg/mL; valproic acid oral solution 200 mg/5 mL; SV tablets 100 mg, 200 mg3.
SV/VA has been associated with multiple adverse effects such as hepatotoxicity, neurotoxicity including psychotic features and hallucinations, headache, abdominal pain, dizziness, hyponatremia, pancreatitis, thrombocytopenia, etc4. The drug has been included under the Schedule H of Drugs and Cosmetics Act, 1940, wherein the drug needs to be prescribed by a Register Medical Practitioner and cannot be sold without a prescription. Over the years, SV/VA related safety concerns in women of childbearing age, particularly birth defects, have been observed and reported5. Within several years after receiving United States Food and Drug Administration (US FDA) approval in the late 1970s, valproate was shown to increase the risk for major congenital malformations and learning disabilities in the offspring of women who used the drug during pregnancy6. The European Medicines Agency (EMA) has taken several initiatives to reduce the risk associated with SV/VA. Countries such as Netherlands, Germany, Finland, Denmark, Australia, Sweden, United States of America (USA), United Kingdom (UK) have reported congenital anomalies due to the maternal use of SV/VA7. France has banned the use of SV during pregnancy, claiming to be the first country in Europe to take such a step8.
The published literature recommends training of both pregnant women taking valproate and the clinicians prescribing them9. The Netherlands and the UK have introduced a special training program for pharmacists for prescription of SV/VA in the childbearing age group women, and consideration of other alternative antiepileptics has been suggested because of the safety issues. The US FDA has also issued a drug safety communication with reference to use of SV/VA and other valproate-related products regarding teratogenic effects like neural tube defects, low IQ and cognitive impairment in children born to SV/VA exposed women10. Women of childbearing age taking valproate should be warned of its teratogenicity and advised to plan pregnancies, take a higher dose of folate, discuss reducing the dose of valproate or changing the medication with their physician, and have antenatal screening. After birth, the infant should be examined for a wide range of reported abnormalities. Neurodevelopmental assessment should continue throughout childhood. The World Health Organization (WHO) through its program for International Drug Monitoring has been continuously involved in education and advocacy for the member states to reduce the risk of SA/VA in women of childbearing age11.
A survey-based questionnaire was developed and circulated to all regional Adverse drug reaction Monitoring Centres (AMCs) across India. The present survey-based study demonstrated the prescribing pattern of SV/VA among the health care professionals (HCPs) for the treatment of epilepsy in women of childbearing age group in India.
Mechanisms of Teratogenicity with SV/VA
Even though a range of potential mechanisms have been reported for SV/VA-induced teratogenicity, including histone deacetylase (HDAC) inhibition and folate antagonism, the exact mechanism is not yet fully understood and several hypotheses have been proposed (Fig. 1). It has been demonstrated experimentally, using enzyme-linked immunosorbent assays (ELISAs) and cell culture modeling that VA serves as a noncompetitive inhibitor of the high affinity folate receptors. Assays in HEK293T cells have shown that the membrane-bound folate receptors of VA treated cells bind significantly lower amounts of folic acid than do untreated cells12. Another proposed theory is the possible influx of proteins monocarboxylate transporter 1 (MCT1) and MCT2, if concentrations are increased or if polymorphisms alter the expression of MCT proteins, the corresponding influx of VA increases maternally and therefore, within the fetus. VA causes chronic impairments in developing human neurons; its exposure alters neuronal properties by inhibiting HDAC and glycogen synthase kinase (GSK)-3 pathways13.
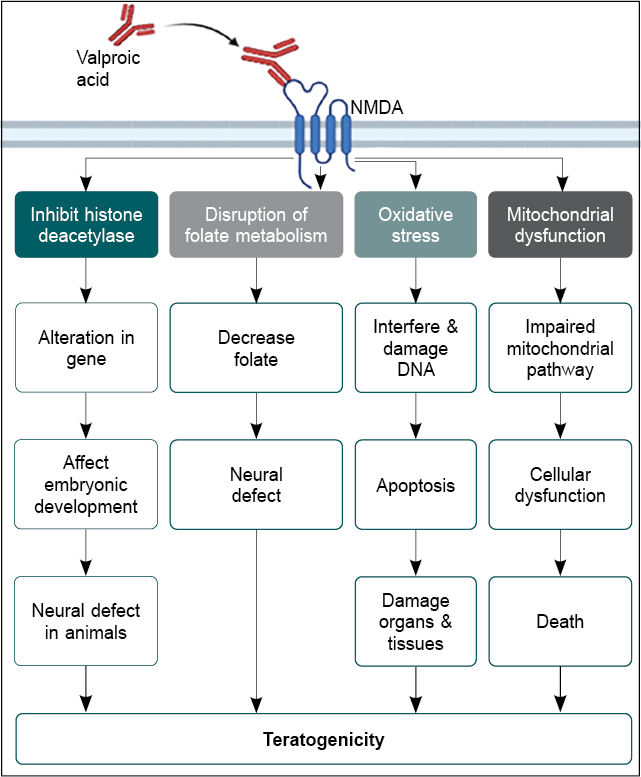
Figure 1. Proposed schematic mechanism of SV/VA-induced teratogenicity.
The cytoskeletal protein myristoylated alanine-rich C-kinase substrate like protein 1 (MARCKSL1) has been proposed to mediate VA-induced morphological defects. A review of studies has shown that intrauterine exposure to VA in rats is associated with changes in hippocampal cell numbers as well as folate metabolism. The mechanism of action is believed to be “neuroprotective” in various disease models such as stroke, neurodegenerative disease or traumatic injury to the central nervous system. However, this effect may not be beneficial during intrauterine development. Because programmed cell death is an important component of normal brain development, VA exposure may interfere with normal embryonically regulated apoptotic programs, resulting in cell type-selective overgrowth that could contribute to the defects observed in VA-exposed off springs14.
The mechanism of SV/VA-induced teratogenicity are as follows:
- Inhibition of HDACs: SV/VA is known to inhibit HDACs, which can lead to alterations in gene expression and affect embryonic development. HDAC inhibition has been shown to cause neural tube defects in animal studies15.
- Disruption of folate metabolism: SV/VA has been shown to decrease folate levels in the body, which is essential for neural tube formation during embryonic development. Low folate levels have been associated with an increased risk of neural tube defects16.
- Oxidative stress: SV/VA has been shown to increase oxidative stress in cells, which can damage DNA and interfere with embryonic development. This oxidative stress can also lead to apoptosis, which can disrupt the normal development of organs and tissues17.
- Mitochondrial dysfunction: SV/VA has been shown to impair mitochondrial function, which can lead to cellular dysfunction and death. Mitochondrial dysfunction has been linked to a range of developmental disorders and may contribute to the teratogenic effects of SV/VA18.
It is important to note that the exact mechanism of SV/VA-induced teratogenicity may be multifactorial and may involve a combination of these mechanisms. Additionally, the risk of teratogenicity may be influenced by factors such as the dose, the timing of exposure and genetic susceptibility. Women of childbearing age who are prescribed VA should be counseled on the potential risks of the medication during pregnancy and advised to use effective contraception19.
The Pharmacovigilance Programme of India at Indian Pharmacopoeia Commission (PvPI-IPC) as the National Coordination Centre (NCC) is also working to reduce the risk of SV/VA. Several educational materials have been developed for this purpose and circulated to all the AMCs across the country for sensitization of the HCPs.
METHODOLOGY
Methods
A questionnaire-based cross-sectional study was conducted to evaluate the outcome of the post-sensitization activities since 2017 regarding the safety of SV/VA use in the women of childbearing age group. A questionnaire was prepared by the NCC-PvPI and circulated via e-mail to all the AMCs across the country. Figure 2 shows the flow of information during the study.
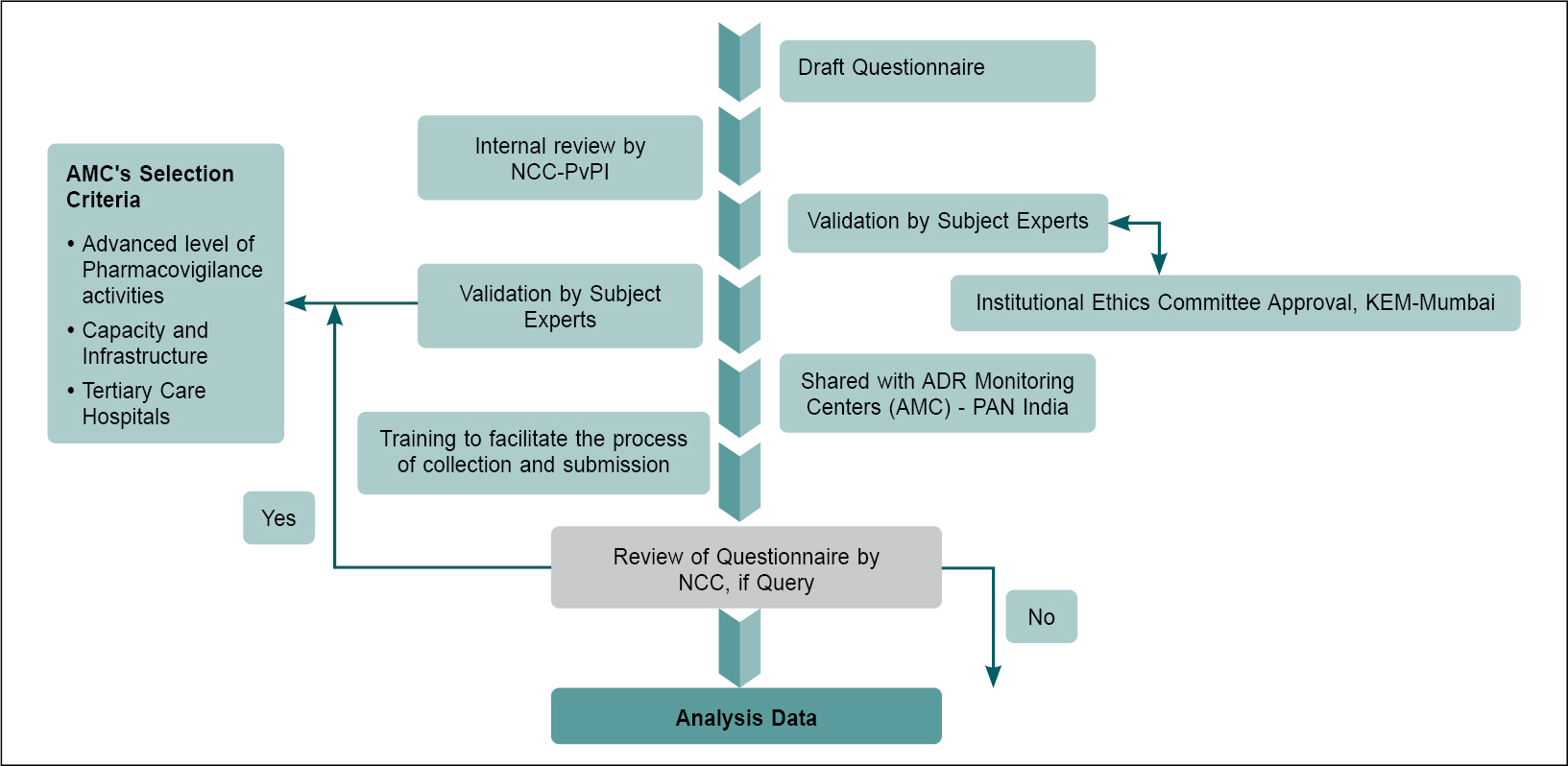
Figure 2. Flow diagram depicting data collection.
Brief About the Questions
The questions were designed on the basis of general information regarding the use of SV/VA in women of childbearing age group, its dose, and any adverse events, which the HCPs had faced during the therapy, etc. Gynecologists/obstetricians and neurologists were selected as participants for this survey study as this was the health care worker population most likely to use SV/VA in pregnant and childbearing age group women.
The details of the participants were kept confidential and their identities were not obtained in their responses (only their qualification as obstetrician/gynecologist or neurologist was obtained). The questions pertaining to the identity of the patient were not added to maintain the confidentiality of the patients.
Questionnaire Validation by Circulation
At the time of the questionnaire circulation, NCC-PvPI had a strong network of 534 AMCs for reporting of adverse drug reactions/adverse events. Of these, 134 AMCs were selected by applying the criteria such as, quality of the specialized care services, quantity and frequency of ADR Reporting and Pharmacovigilance Capacity at the Centre (Fig. 2).
The questionnaire was validated by trained and skilled Pharmacovigilance teams at the AMCs and 10 questions were finalized focusing the prescribing pattern, adverse event reporting and preventive measures for SV/VA use in childbearing age group women. The NCC-PvPI provided study assistance to the PvPI team at the AMCs so that they could complete the questionnaire as planned.
Period of study
The study was conducted from 2017 to 2022 and the survey was open for the 6 months from December 2021 to June 2022.
Ethics Committee approval
The approval for the study was obtained from Institutional Ethics Committee (IEC)-I relating to Biomedical and Health Research (BHR), Seth GS Medical College and KEM Hospital, Mumbai, Maharashtra, India, with the registration Number EC/OA-51/2022.
VigiLyze
During the same study period, we also attempted to analyze the trend or pattern of SV/VA adverse event reporting from these centers. The VA/SV safety data was extracted from VigiLyze. These data showed that there was a significant decreasing trend in the pattern of SV/VA individual case safety reports (ICSRs) in women of childbearing age (Fig. 3).
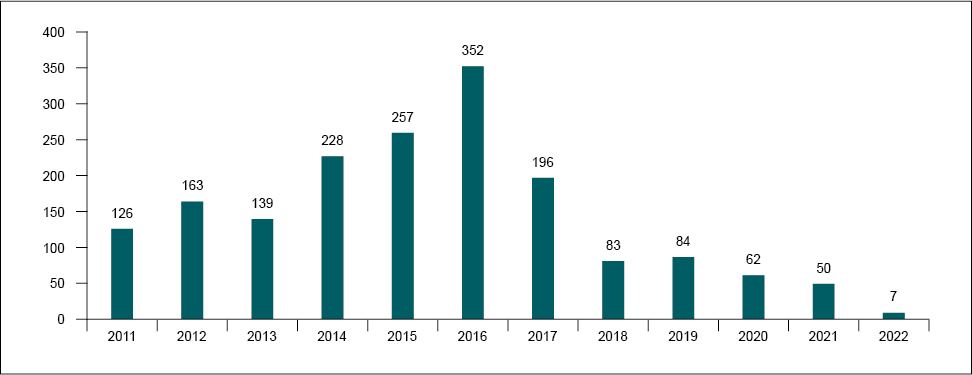
Figure 3. VigiLyze displayed significant decreasing trend in the pattern of SV/VA ICSRs.
RESULTS
Out of 134 AMCs, 41 AMCs responded to the questionnaire, which included a total of 251 responses from HCPs. Out of these, 50 responses were obtained from gynecologists/obstetricians, 22 from neurologists, and 179 from the interns/resident doctors in the AMCs. There were 93 responses in which it was mentioned that SV is not being used by that HCP.
- Have you ever noticed any adverse event(s) associated with the use of SV/VA in the women of childbearing age (18-40 years)?
Yes No
Reply: One hundred eighty-seven HCPs mentioned that they had not noticed any adverse event(s), while 61 HCPs had noticed. Three HCPs did not provide any response (Fig. 4).
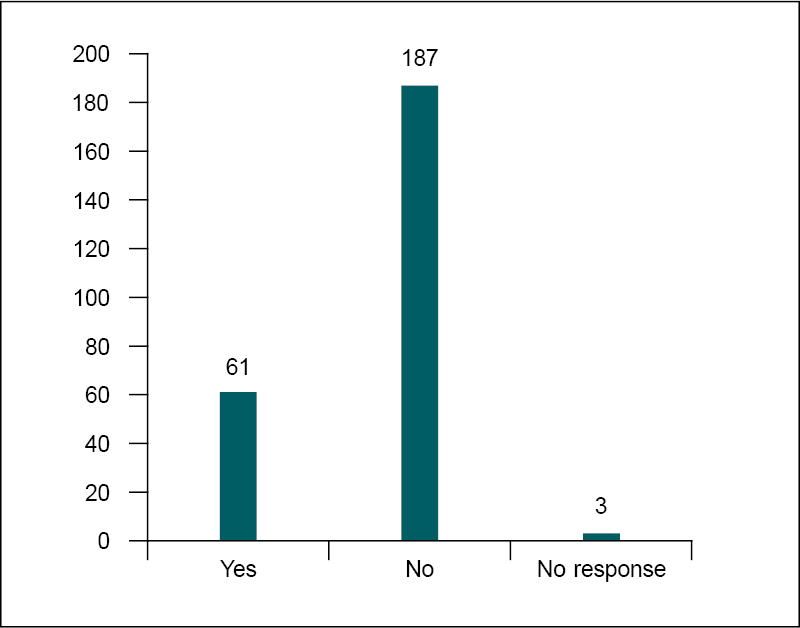
Figure 4. Significant numbers of HCPs had never noticed any adverse events with SV/VA in women of childbearing age group.
- If yes, have you reported this to AMC/Regional Centre/National Pharmacovigilance Centre?
Yes No
Reply: Only 22 HCPs had mentioned that they reported such events to Regional AMCs. However, 149 respondents mentioned that they had not reported and 75 left the question blank (Fig. 5).
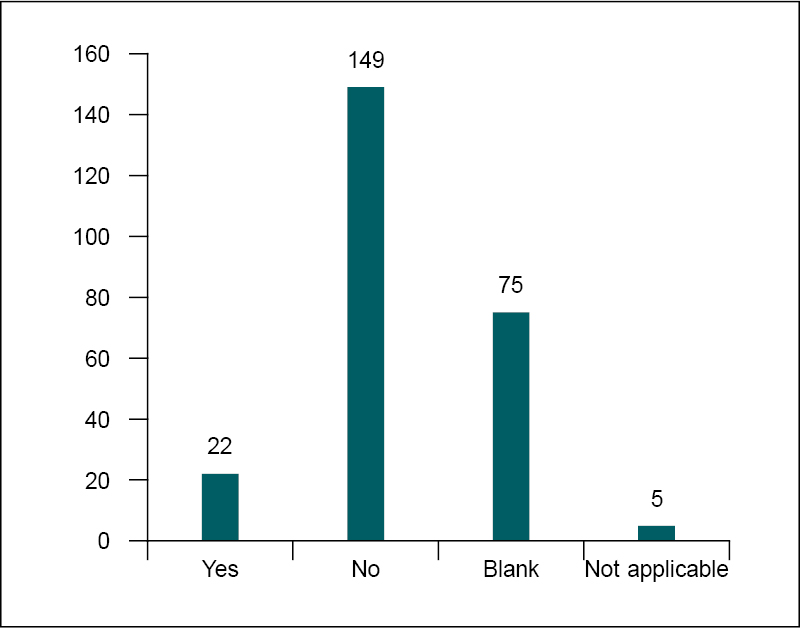
Figure 5. Reporting of adverse events with the use of SV/ VA to AMCs.
- If yes, what common adverse effects have you come across related to SV/VA among the women of child bearing age?
Birth Defects Others_____________________
(Please specify the adverse events if any in maternal or neonatal)
Reply: There were 20 reports of birth defects and related events, 6 fetal bradycardia, 6 polycystic ovary syndrome, 10 events of weight gain and 4 events of alopecia. Abdominal discomfort, gingival hyperplasia, increase in liver enzyme, gastritis, menstrual irregularities, acneiform eruptions, neurodevelopmental disorder, gingival enlargement, spina bifida, headache, drowsiness, tremors, dizziness, vomiting, weakness were the other infrequent events reported due to use of SV/VA in women of childbearing age.
- What about the dose, duration, and frequency of administration of SV/VA to cause the adverse event(s) mentioned in question number 3?
Dose of SV/VA________________________________
Frequency of administration____________________
(Please specify the dose administered for total number of days/months/years/duration of treatment)
Reply: The SA/VA was taken by the patients as per the standard dosage regimens for respective indications.
- The adverse events with the use of SV/VA have been noticed in childbearing age group of women but could not be reported because of
Time constraint
Legal issues
Unwillingness
Not aware of where to report
Others _______________________________________
Reply: Thirty-three ADRs were not reported by the HCPs because of time constraints, 4 HCPs were avoiding reporting due to the fear of legal issues, 13 HCPs were not willing to report, 35 HCPs were not aware of where to report, and 128 HCPs had other reasons (Fig. 6).
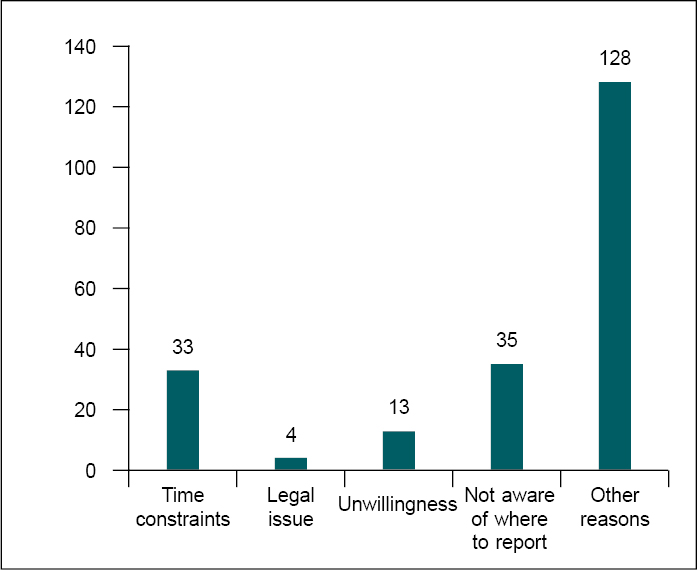
Figure 6. Significant numbers of HCPs were not reported.
- Due to the adverse events associated with the SV/VA among this special age group, did you prescribe any alternate drug?
Yes No
Reply: One hundred (100) HCPs responded that they had started prescribing an alternative medicine to SV/VA due to the ADR, while 86 HCPs still continued with SV/VA. The remaining did not respond.
- If yes, name those drugs below:
Alternate drugs ______________________________
Reply: As an alternative medicine to sodium valproate, medicines prescribed by HCPs were as enumerated in Box 1.
|
Box 1. Alternative Drugs Prescribed by the HCPs
|
|
Olanzapine
|
Carbamazepine
|
|
Risperidone
|
Phenytoin
|
|
Lamotrigine
|
Flunarizine
|
|
Oxcarbazepine
|
Propranolol
|
|
Levetiracetam
|
|
- When did you start prescribing alternative drugs?
- After alert/educational materials received from National Pharmacovigilance Centre or WHO
- Based on my own clinical judgment
- Others (please specify)
Reply: Twelve HCPs started prescribing alternative drugs after awareness received from National Pharmacovigilance Centre or WHO, while 110 HCPs prescribed them based on their own clinical judgment.
- How did you share the experiences related to SV/VA safety in childbearing age group women to the HCPs and others?
- Seminar/trainings/meetings/social media campaigns
- Not shared because________________________(you may specify the reason)
Reply: One hundred two HCPs had shared the WHO and IPC newsletters and bulletins among their colleagues via seminar/meetings, etc. to disseminate the information, whereas 149 number HCPs applied their own clinical experiences for not using the SV.
DISCUSSION
Up to April 2022, 93 of the 134 centers contacted did not complete the questionnaire because they said the drug was not in use in the centers since the guidance was issued in 2016.
The responses showed that only 20 of the 58 HCPs (34.5%), who observed an ADR in women aged 18 to 40, reported the event. The reasons for not reporting included: did not know where to report (16.6%), time constraints (13.3%), unwillingness (6.2%), and legal issues (2.1%). The most frequent ADRs concerned birth defects. The dose and frequency of administration reported varied widely: 200 mg/day to 2,000 mg, QD or BID or TID with duration from 7 days to 3 years.
A total of 100 HCPs reported they had prescribed an alternative treatment because of the adverse events associated with SV/VA. These treatments included carbamazepine, lamotrigine, levetiracetam, oxcarbazepine, olanzapine, propranolol, and second-generation antipsychiatric drugs.
Out of 116 respondents, 71 started prescribing alternative medication based on their clinical judgment, 24 followed the alert of educational materials received from their National Pharmacovigilance Centre or WHO, and 21 during the study. Out of 142 respondents, 94 shared their experience with safety of valproate containing treatments in women of childbearing age through seminars, training, meetings, and social media, 7 shared during ward rounds and clinical teaching and the remaining 41 did not share for a variety of reasons including no permission from department head, or legal reasons.
The WHO has advised about the safety and use of SV/VA in childbearing age group, particularly events related to birth defects20. The IPC, NCC-PvPI has published several IEC materials for stakeholders about the risk associated with SV/VA use in women of childbearing age group. Subsequent to this advisory from NCC-PvPI, we found that there was a decrease in the ICSRs reporting among the childbearing age group women in the Indian database. This can be attributed to compliance with NCC-PvPI Advisory.
However, a decreased overall reporting by chance or other reasons could also have occurred. The responses reveal that 40% were aware and 60% were unaware of SV/VA teratogenic effects. Around 37% of HCPs involved in the study stated that they were not using the drug. The IEC material for Pharmacovigilance played an important role in creating awareness amongst HCPs and other stakeholders.
LIMITATION OF STUDY
The study is limited to two departments, i.e., Gynecology and Neurology. The reason of including these two departments was that the exposure of SV/VA is generally expected to be maximum in these two departments.
Another limitation that the response to the questionnaire was poor among the AMCs despite multiple reminders (only 41 out of 134 AMCs responded). The use of option ‘others’ in the questionnaire was not properly answered by the responders.
CONCLUSION
The data shows that the efforts of IPC, NCC-PvPI through Resource Material (i.e., Newsletter, Posters, Advisory, etc.), training, seminars, etc. might have resulted in a decrease in the trend of ICSRs with use of SV/VA in women of childbearing age group.
Nevertheless, on account of the low awareness levels regarding reporting of ADRs and the availability of IEC materials, further strategies need to be developed to improve the penetration of NCC-PvPI activities at the level of the AMCs. This data can help in promoting the safe use of SV/VA and taking appropriate steps for protecting the safety of vulnerable population at the global level. IPC as a WHO Collaborating Centre will support WHO to expand/initiate this survey-based questionnaire study to its member states.
Competing Interests
Nil conflict of interest.
Funding
Not applicable.
Availability of Data and Materials
The data is available in the form of soft copy received from various health care professionals.
REFERENCES
- Chang ZL. Sodium valproate and valproic acid. Anal Profiles Drug Subst Excipients. 1979;8:529-56.
- Seshachala BB, Jose M, Lathikakumari AM, Murali S, Kumar AS, Thomas SV. Valproate usage in pregnancy: An audit from the Kerala Registry of Epilepsy and Pregnancy. Epilepsia. 2021;62(5):1141-7.
- IPC, NCC-PvPI, News Letter, Drug Safety Review: Valproic acid use in pregnancy: A necessity of precaution and Pharmacovigilance in India. 2016;6(17):4-5.
- Rahman M, Awosika AO, Nguyen H. Valproic Acid. [Updated 2023 Aug 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559112/.
- Macfarlane A, Greenhalgh T. Sodium valproate in pregnancy: what are the risks and should we use a shared decision-making approach? BMC Pregnancy Childbirth. 2018;18(1):200.
- Gruppuso PA, Ahmed R, Adashi EY. Valproate teratogenicity: a moving target. Obstet Gynecol. 2022;140(3):408-11.
- Jentink J, Loane MA, Dolk H, Barisic I, Garne E, Morris JK, et al; EUROCAT Antiepileptic Study Working Group. Valproic acid monotherapy in pregnancy and major congenital malformations. N Engl J Med. 2010;362(23):2185-93.
- Casassus B. France bans sodium valproate use in case of pregnancy. Lancet. 2017;390(10091):217.
- Smith J, Whitehall J. Sodium valproate and the fetus: a case study and review of the literature. Neonatal Netw. 2009;28(6):363-7.
- US FDA. Valproate Information. Published October 7, 2015. Available from: https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/valproate-information. Accessed April 28, 2024.
- Programme for International Drug Monitoring. Available from: https://www.who.int/teams/regulation-prequalification/regulation-and-safety/pharmacovigilance/networks/pidm. Accessed April 28, 2024.
- Fathe K, Palacios A, Finnell RH. Brief report novel mechanism for valproate-induced teratogenicity. Birth Defects Res A Clin Mol Teratol. 2014;100(8):592-7.
- Alsdorf R, Wyszynski DF. Teratogenicity of sodium valproate. Expert Opin Drug Saf. 2005;4(2):345-53.
- Semmler A, Frisch C, Bleul C, Smith D, Bigler L, Prost JC, et al. Intrauterine valproate exposure is associated with alterations in hippocampal cell numbers and folate metabolism in a rat model of valproate teratogenicity. Seizure. 2017;46:7-12.
- Menegola E, Di Renzo F, Broccia ML, Giavini E. Inhibition of histone deacetylase as a new mechanism of teratogenesis. Birth Defects Res C Embryo Today. 2006;78(4):345-53.
- Greene ND, Copp AJ. Neural tube defects. Annu Rev Neurosci. 2014;37:221-42.
- Graf WD, Oleinik OE, Glauser TA, Maertens P, Eder DN, Pippenger CE. Altered antioxidant enzyme activities in children with a serious adverse experience related to valproic acid therapy. Neuropediatrics. 1998;29(4):195-201.
- Chen H, Dzitoyeva S, Manev H. Effect of valproic acid on mitochondrial epigenetics. Eur J Pharmacol. 2012;690(1-3):51-9.
- Tomson T, Battino D, Bromley R, Kochen S, Meador K, Pennell P, et al. Management of epilepsy in pregnancy: a report from the International League Against Epilepsy Task Force on Women and Pregnancy. Epileptic Disord. 2019;21(6):497-517.
- WHO recommendations on antenatal care for a positive pregnancy experience. Geneva: World Health Organization; 2016. Available from: https://www.who.int/publications/i/item/9789241549912. Accessed April 28, 2024.