It has been 70 years since the term
‘noncommunicable disease’ (NCD) was first used in medical literature1.
The importance of noninfectious chronic diseases, however, was understood much
earlier. The death of President Roosevelt, from an untimely stroke, was one
factor which spurred investment in research on this topic2. The
Framingham Heart Study, which later led to the concept of ‘risk factors’, was
an outcome of this interest3.
Over the past few decades, the scope and
spectrum of NCD has changed and evolved. To bring clarity to an ever-expanding
field, the World Health Organization (WHO) created a 4 × 4 framework, listing 4
major NCDs and 4 major risk factors4. This simple rubric facilitated
a global movement on NCD prevention and management. While the diseases were
chosen for their clinical and public health impact - diabetes, cardiovascular
disease, cancer, and chronic respiratory diseases, the 4 risk factors
(unhealthy diet, physical inactivity, tobacco, and alcohol) were listed as they
are common to all the aforementioned disorders.
There has been criticism of the 4 × 4 framework,
as it excludes many important diseases. There have also been calls to modify it
to a 5 × 5 framework, with mental health and oral health claiming their place
under the NCD sun5. It must be remembered, however, that the NCD
campaign is a relatively recent one, and major changes to its taxonomy may
confuse the intended audience rather than consolidate our efforts.
At the same time, innovation and improvement are
an integral part of science, and we must continually strive to do better. In
recent years, obesity has emerged as an opportunity for prevention of disease,
and promotion of health. Obesity is recognized as a disease in itself, and is
also a forerunner of all the conditions6-8 listed in the 4 × 4 WHO
NCD framework. It shares the same risk factors, and should respond to similar
public health interventions as these diseases. The health economic impact of
the obesity pandemic, and the financial savings that may accrue if we are able
to arrest it, are significant9.
It is logical, therefore, to call for a minor
adjustment to the existing 4 × 4 framework. We suggest a reframing of this
rubric, by adding obesity at the center (Fig. 1), and naming it the 4-1-4
framework. This seemingly simple change will have far-reaching beneficial
effect on public as well as clinical health. Governments and other
stakeholders will be able to focus efforts on the upstream opportunity of
obesity, and prevent downstream disorders such as cardiometabolic disease and
cancer, with a single intervention. Physicians and paramedical staff will be
able to redouble their efforts to fight obesity and overweight, using a
standard WHO reference point. Other stakeholders, such as insurance payers and
non-governmental organizations will be able to support delivery of accessible
and affordable obesity care. Most important of all, the public, which is
perhaps the most important player, will realize the importance of overcoming
obesity, and begin to act accordingly.
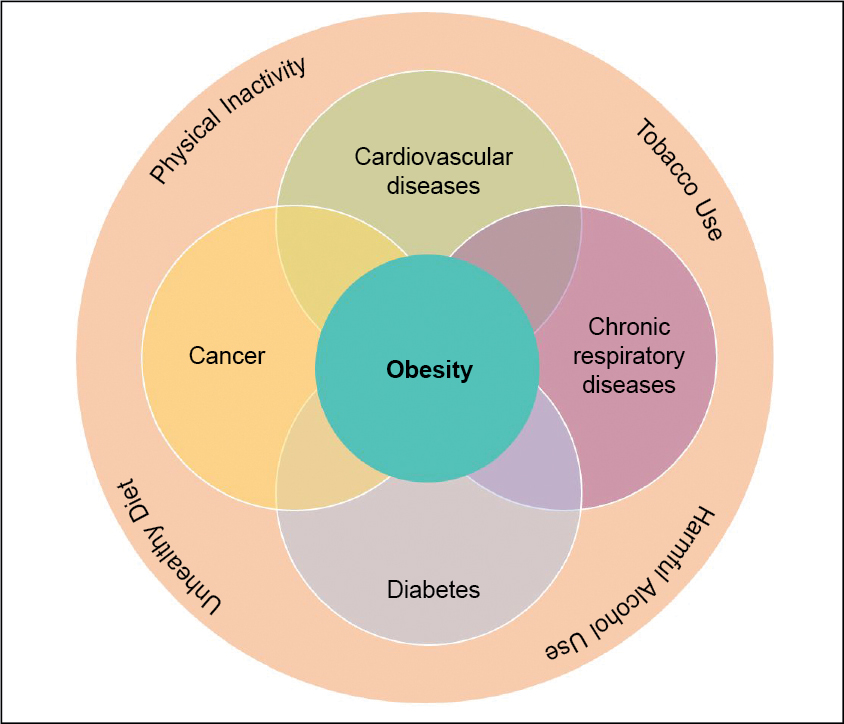
Figure 1.
To have a healthier future, for ourselves, and
for future generations, we must adopt the 4-1-4 framework. Obesity is an
obstacle to health that we should not be oblivious to; at the same time obesity
management is an opportunity, which we must not overlook.
1.
Gilliam AG. Epidemiology in noncommunicable disease. Public Health Rep (1896). 1954;69(10):907-13.
2.
Adjaye-Gbewonyo K, Vaughan M. Reframing NCDs? An analysis of current debates. Global Health Action. 2019;12(1):1641043.
3.
Kannel WB, Dawber TR, Kagan A, Revotskie N, Stokes J 3rd. Factors of risk in the development of coronary heart disease—six-year follow-up experience: the Framingham Study. Ann Intern Med. 1961;55(1):33-50.
4.
Schwartz LN, Shaffer JD, Bukhman G. The origins of the 4 × 4 framework for noncommunicable disease at the World Health Organization. SSM Popul Health. 2021; 13:100731.
5.
Mensah GA, Mayosi BM. The 2011 United Nations high-level meeting on non-communicable diseases: the Africa agenda calls for a 5-by-5 approach. S Afr Med J. 2013;103(2):77-9.
6.
Conway B, Rene A. Obesity as a disease: no lightweight matter. Obes Rev. 2004;5(3):145-51.
7.
S V M, Kapoor N, Das S, Raizada N, Kalra S; (on behalf of Endocrine Society of India). ESI clinical practice guidelines for the evaluation and management of obesity in India. Indian J Endocrinol Metab. 2022;26(4):295-318.
8.
Kalra S, Kapoor N, Verma M, Shaikh S, Das S, Jacob J, et al. Defining and diagnosing obesity in India: a call for advocacy and action. J Obes. 2023;2023:4178121.
9.
Nagi MA, Ahmed H, Rezq MAA, Sangroongruangsri S, Chaikledkaew U, Almalki Z, et al. Economic
costs of obesity: a systematic review. Int J Obes (Lond). 2024;48(1):33-43.