Abstract
Laparoscopic
cholecystectomy (LC) is the gold standard treatment for gallstones. Since its
inception in 1987, it has undergone various changes, with reduced number of
ports from standard 4-port LC to 3-port LC being one of them. Three-port LC has
been shown to be equal to standard 4-port LC in terms of safety, complications,
pain and hospital stay. We conducted a prospective comparative study amongst
these two techniques. Three-port LC was found to be superior in terms of less
postoperative pain, less need of analgesia, shorter hospital stay and ease of
dissection. We concluded that 3-port LC is a better operative technique than
4-port LC.
Keywords: Three-port laparoscopic cholecystectomy, benefits, safety
Standard
laparoscopic cholecystectomy (LC) is done by using 4 trocars. Exposing Calot’s
triangle for satisfactory anatomical details is of paramount importance in safe
and proper surgery. The fourth (lateral) trocar is used to grasp the fundus of
the gallbladder so as to expose Calot’s triangle. The use of the fourth trocar,
which is generally used for retraction of the fundus in the American technique,
was found unnecessary by some surgeons1 and LC can be performed
safely without using it. With widespread advent of LC, comes the advent of
reduction in port size2. Most of these studies have demonstrated the
advantages of 3-port LC including less postoperative pain, early hospital
discharge and less analgesic requirement. We did a prospective comparative
clinical study to investigate the safety, and benefit of 3-port LC versus
standard 4-port LC in our setup. Benefits associated with 3-port LC were
compared in terms of pain on visual analog scale (VAS), requirement of
analgesia and hospital discharge.
This was a comparative prospective study
performed in the Dept. of Surgery, from January 2014 to January 2015. A total
of 50 patients, diagnosed to have gallstone disease and confirmed on ultrasound
examination, who were willing to participate in the study and gave valid
consent, were included in the study. They were allocated into two groups of
3-port LC and 4-port LC with 25 patients in each group.
Exclusion
Criteria
Patients with suspected common bile duct stones,
history of obstructive jaundice, gallstone pancreatitis, acute cholecystitis.
Preoperative work-up was carried out, which
included complete history, clinical examination, and standard laboratory
investigations for the fitness for surgery, including ultrasonography of
abdomen and liver function tests.
In standard 4-port technique, one 10 mm
umbilical port for camera was made after creating capnopneumoperitoneum with
closed technique, another 10 mm epigastric port 5 cm below the xiphisternum
(main working port), one 5 mm port in the right midclavicular line 5 cm below
the right costal margin (accessory working port) and another 5 mm port, i.e.,
the fourth port in the right anterior axillary line at the level of umbilicus
were used. In 3-port technique, the 4th port (which was put at right anterior
axillary line at the level of umbilicus) was not used (Fig. 1).

Figure 1. Three-port positions.
The outcomes were measured in terms of operating
time, conversion rate, intraoperative complications, pain score, analgesic
requirement, and hospital stay. Intraoperative complications include
gallbladder wall perforation, bile leak, bleeding from liver bed, iatrogenic
liver injury, and bile duct injury. In all patients, the same analgesics were
used. Pain score was measured using VAS every 12 and 24 hourly. A VAS score 1-3
is called as low pain score (mild) and 4-10 as high pain score (severe).
Statistical
Analysis
The Student’s t-test was used to evaluate
the difference in each parameter. A p value <0.05 was considered
statistically significant. Statistical package for Social Science version 19.0
for Windows (SPSS, Chicago, Illinois) was used for statistical analysis.
On comparing the two groups, we made the
following observations (Table 1):
·
Operating time: Mean operating time was 38.3 minutes in 3-port group while it was 41.0 minutes in the 4-port group. There was no significant difference in operating time in our study (p = 0.06).
·
Conversion rate: Both the groups were equal in terms of conversion rate as it was zero in both of them.
·
Intraoperative complications: There were two gallbladder wall perforations in 4-port group and no perforation in 3-port group; this was statistically significant (p = 0.02). There was no bleeding from liver bed on comparing both groups,
no iatrogenic liver injury in both the groups and fortunately no bile duct injury was found.
·
Pain score: VAS on the scale of 1-10 was used. Mean score in 3-port group was 1.8, while it was 2.9 in 4-port group. This was statistically significant (p = 0.01). Three-port group had better outcome in terms of 4-port group when compared
on the basis of VAS. The more pain experienced in 4-port group was probably due to more tissue trauma while putting the 4th port and putting the visceral peritoneum on more stretch.
·
Analgesic requirement: Analgesic requirement was high in 4-port group. Patients in 4-port group required 5.2 injection of IV diclofenac 75 mg/2 mL/patient, while the mean requirement in 3-port group was of 3.6 injections/patient. This
was statistically significant (p = 0.001), hence the analgesic requirement was significantly less in 3-port group.
·
Hospital stay: Mean hospital stay was 1.3 days in 3-port group as most of the patients were discharged on the next day of surgery and it was 2.4 days in 4-port group.
|
Table 1. The Overall Endpoints of the Study
|
|
Findings
|
3-Port group
|
4-Port group
|
P value
|
|
Operating time (minutes)
|
38.3
|
41.0
|
0.06 (not significant)
|
|
Conversion rate
|
Nil
|
Nil
|
NA
|
|
Intraoperative complications
|
|
Perforation of gallbladder only
|
0
|
2
|
0.02 (significant)
|
|
Bleeding
|
0
|
0
|
NA
|
|
Hepatobiliary injuries
|
0
|
0
|
NA
|
|
Pain score
|
1.8
|
2.9
|
0.01 (significant)
|
|
Analgesic requirement (number)
|
3.6
|
5.2
|
0.001 (significant)
|
|
Hospital stay (days)
|
1.3
|
2.4
|
0.02 (significant)
|
At present, LC is the treatment of choice for
gallbladder stones3. Less postoperative pain and early recovery are
major goals to achieve better patient care and cost-effectiveness. These goals;
however, cannot be compromised for patient safety. Since Slim et al reported
that 4th port is not necessary in their 710 cases of LC, several studies have
shown the technical feasibility, safety, less pain, and early hospital
discharge with the 3-port LC4,5. In our study, we demonstrated that
the advantages of 3-port LC were less intraoperative complications (perforation
of gallbladder only), less pain, significantly reduced need for
analgesia, and shorter hospital stay. Operating time was not significantly
different in the two groups in our study.
In our experience, perforations of gallbladder
while dissection occurred in 4-port group because of undue and strong traction
on fundus of gallbladder by assistant; there is more stretch on the tissues of
gallbladder making them prone to perforation. Most of the studies comparing
these two techniques conclude that there are either no or equal intraoperative
complications, but we could prove that gallbladder perforation and subsequently
bile spillage was more in 4-port group. Another surgical aspect that we
observed is that the operating surgeon has full control while doing dissection
of Calot’s triangle and posterior and anterior peritoneal folds were dissected
easily. So, skeletonization of cystic duct and artery becomes very easy,
because there is no stretch on gallbladder and it is more mobile for dissection
(Figs. 2 and 3).

Figure 2. Cystic duct completely dissected in Calot's
triangle.
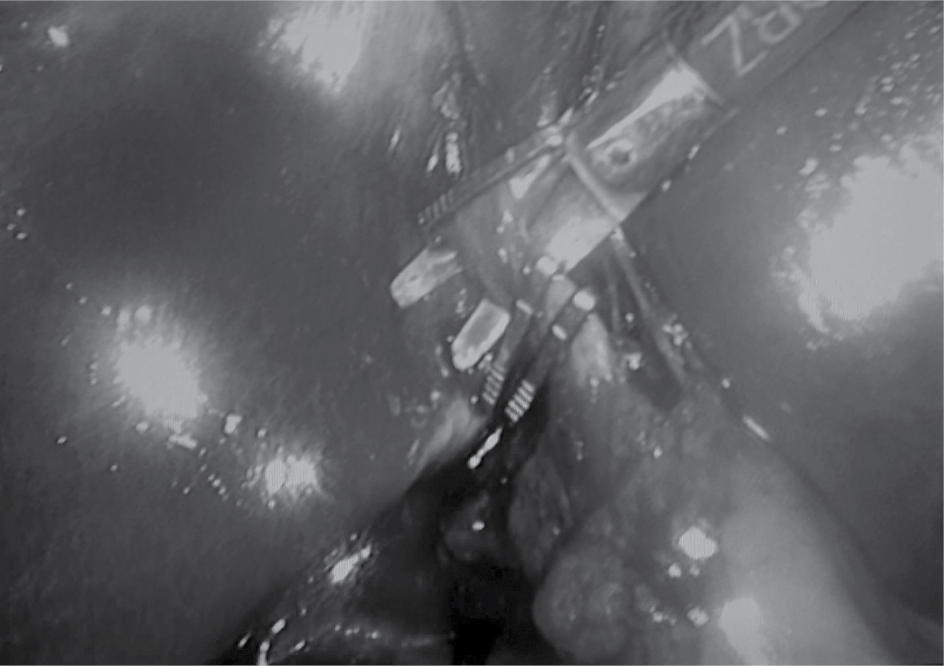
Figure 3. Cystic duct clipped and ready to be cut;
cystic artery seen at the back of scissor.
Less pain and significant reduction of analgesia
has been a strong push for reduced port surgery. Our study is in accordance
with most of the other studies2,5-7. Less tissue dissection in
abdominal wall, low stretch on visceral peritoneum significantly reduce the
postoperative pain and shorten the hospital stay.
Significant reduction in pain and requirement of
analgesia translates into shorter hospital stay in 3-port LC group. The
reduction in hospital stay has been proved by many of the studies5,7.
Three-port LC technique is easy to perform as compared to 4-port LC and
can be safely performed after good training in LC.
We conclude that the 3-port LC technique is
feasible, safe and has better outcomes as compared to those of the standard
4-port LC in terms of postoperative pain, need for analgesia, and shorter
hospital stay. The surgical technique is easy and dissection much easier.
It is a better technique over 4-port LC.
1.
Osborne D, Boe B, Rosemurgy AS, Zervos EE. Twenty-millimeter laparoscopic cholecystectomy: fewer ports results in less pain, shorter hospitalization, and faster recovery. Am Surg. 2005;71(4):298-302.
2.
Kumar M, Agrawal CS, Gupta RK. Three-port versus standard four-port laparoscopic cholecystectomy: a randomized controlled clinical trial in a community-based teaching hospital in eastern Nepal. JSLS. 2007;11(3):358-62.
3.
Soper NJ, Stockmann PT, Dunnegan DL, Ashley SW. Laparoscopic cholecystectomy. The new ‘gold standard’? Arch Surg. 1992;127:917-21.
4.
Slim K, Pezet D, Stencl J Jr, Lechner C, Le Roux S, Lointier P, et al. Laparoscopic cholecystectomy: an original three-trocar technique. World J Surg. 1995;19(3):394-7.
5.
Harsha HS, Gunjiganvi M, Singh AK, Moirangthem GS. A study of three-port versus four-port laparoscopic cholecystectomy. J Med Soc. 2013;27(3):208-11.
6.
Hashimoto D, Hirota M, Yagi Y, Baba H. Umbilicus saving three-port laparoscopic cholecystectomy. WebmedCentral
Laparoscopy. 2011;2(4):WMC001882.
7.
Al-Azawi D, Houssein N, Rayis AB, McMohan D, Hehir DJ. Three-port versus four-port laparoscopic cholecystectomy in acute and chronic cholecystitis. BMC Surg. 2007,7;8.