Dear Sir,
A 64-year-old male presented with hoarseness of
voice for past 9 months. Direct laryngoscopy showed that the left vocal cord
had a proliferative growth was extending into the subglottis. The left vocal
cord was fixed. The biopsy of this lesion was suggestive of carcinoma larynx.
He was planned for total laryngectomy and bilateral neck dissection under
general anesthesia. His past history was notable for coronary artery diseases
for which he had undergone coronary angioplasty. He had a stent in left anterior
descending artery, an ejection fraction of 35%-40% and a pacemaker was in situ.
Prior to the surgery, central venous access was established by inserting a
right subclavian line by infraclavicular approach as per standard protocol1.
The subclavian venous access had been confirmed by a flash of blood and a
nonpulsatile drip of blood upon removing the needle, prior to inserting the
catheter. A check radiograph was done after the procedure which confirmed the
correct position of the line (Fig. 1).
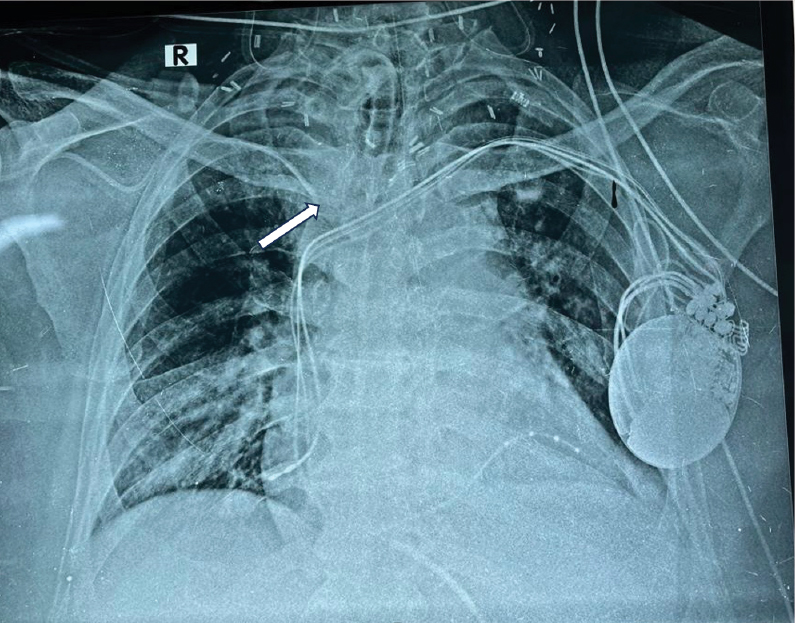
Figure 1. Initial check radiograph showing appropriately
positioned subclavian venous catheter (white arrow).
The surgery was uneventful and after surgery,
the anesthesia was reversed and the patient was breathing spontaneously from
the tracheostomy tube. On postoperative day 1, the patient complained of
swelling in the neck which was present diffusely around the surgical site and
extending towards the chest. The surgeons noted serosanguineous discharge from
the drain placed at the surgical site in the neck. The discharge continued till
the next day and the surgeons were not sure of the cause. Accordingly, a surgical
re-exploration was planned. The patient was shifted to the operating room and
general anesthesia was being induced. The anesthetist who was administering the
anesthesia, noted that immediately after injecting propofol, a milky white
fluid was observed in the drain. Suspecting the obvious, the surgery was put on
hold and a neck radiograph was ordered immediately. The radiograph revealed
that the central line had malpositioned and its tip was seen at the level of
clavicle in the radiograph, probably lying in the subcutaneous space (Fig. 2).
As a consequence of this, intravenous fluid being given to the patient had been
leaking into surrounding tissues – the same was appearing in the surgical drain
as well as causing local edema. There was no evidence of any mediastinal
collection or pneumothorax or hydrothorax. The central line was promptly
removed and the surgery was canceled. By the next day, the swelling had
subsided and the drain showed minimal output. The patient was discharged after
2 days.
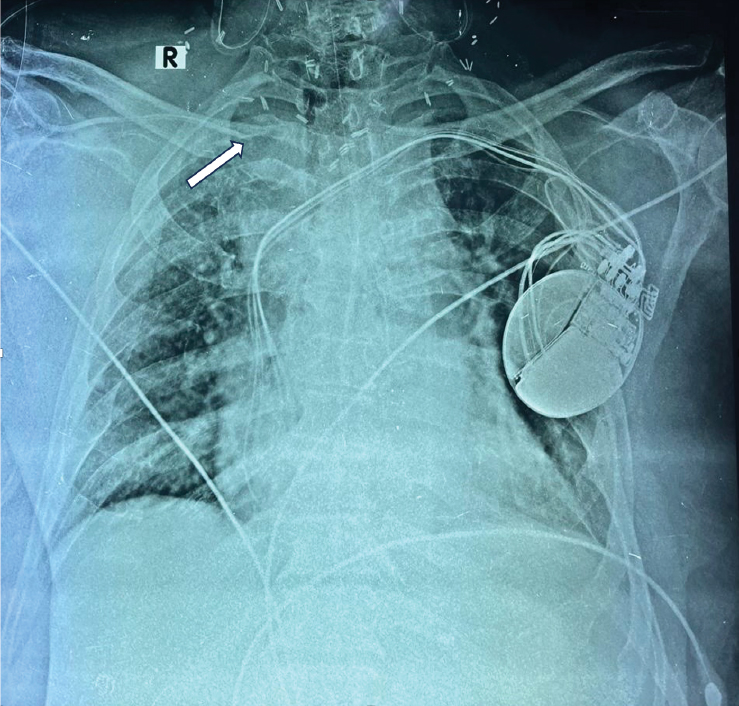
Figure 2. Radiograph taken on postoperative day 2 after
noting intravenous propofol appearing in surgical drain showing catheter
malposition (white arrow).
Subclavian vein catheterization is a common
procedure performed often for perioperative fluid management, giving
chemotherapy, total parenteral nutrition or long-term antibiotics.
Complications in subclavian vein catheterization are not uncommon and around
10% cases can have complications2.The complications can
be immediate such as catheter misplacement, cardiac arrhythmia, arterial
puncture, pneumothorax, pneumomediastinum, bleeding, mediastinal hematoma,
guidewire or catheter entanglement or entrapment apart from several others3,4.
Delayed complications include infections and catheter blockade due to fibrin
sheath, thrombosis or catheter fracture. Misplacement was the most common
complication in one study, seen in 6% of cases2.
The misplacement related complications are
usually noted immediately and are almost always detectable by performing a
check radiograph. In our case, there does not appear to be an immediate
misplacement as the catheter was working normally and the radiograph was also
showing appropriate placement. The malposition of the catheter appears to have
occurred after surgery. Under normal circumstances, swelling around the
catheter insertion site would have been a dead giveaway of leakage but in our
case since the surgical site was nearby and the surgical drain was showing a
collection, a surgical complication was suspected. The chance noting of the
propofol appearing in the drain by the anesthetist averted an unnecessary
surgery. Delayed malposition of subclavian vein catheter appears to a rare
complication about which the anesthetists should be aware.
1.
Kilbourne MJ, Bochicchio GV, Scalea T, Xiao Y. Avoiding common technical errors in subclavian central venous catheter placement. J Am Coll Surg. 2009;208(1):104-9.
2.
Mansfield PF, Hohn DC, Fornage BD, Gregurich MA, Ota DM. Complications and failures of subclavian-vein catheterization. N Engl J Med. 1994;331(26):1735-8.
3.
Kumar P. Ultrasound-guided subclavian vein cannulation using open door technique - A technical report. Indian J Anaesth. 2023;67(12):1133-4.
4.
Imai E, Watanabe J, Okano H, Yokozuka M. Efficacy and safety of supraclavicular versus infraclavicular approach for subclavian vein catheterisation: an updated syst
ematic review and meta-analysis of randomised controlled trials. Indian J Anaesth. 2023;67(6):486-96.