Abstract
Background: Dual antiplatelet therapy (DAPT),
consisting of aspirin, and a P2Y12 inhibitor, has been crucial for reducing
ischemic events following percutaneous coronary intervention (PCI). However, the
optimal duration of DAPT remains under investigation. Objective: This
meta-analysis aims to compare the efficacy and safety of an
abbreviated-duration DAPT (Abv-DAPT) regimen (ticagrelor plus aspirin for 1
month or less, followed by ticagrelor monotherapy) with a conventional
long-term duration DAPT (L-DAPT) regimen (ticagrelor plus aspirin for 12
months) in patients who have undergone PCI. Methods: We systematically
searched PubMed-MEDLINE, EMBASE, Scopus, and the Cochrane Central Registry of
Controlled Trials for studies with cohorts of patients who had undergone PCI
and received DAPT with ticagrelor and aspirin. We analyzed data from the
ULTIMATE-DAPT, T-PASS, and GLOBAL-LEADERS trials. Efficacy outcomes for this
analysis were all-cause mortality, myocardial infarction, stent thrombosis, and
stroke. Safety outcomes were major bleeding. The efficacy and safety events in
patients of the Abv-DAPT arm were compared with those of L-DAPT arms. Results:
The consolidated population from three major trials included in the
meta-analysis was 22,218, with a nearly equal distribution between the Abv-DAPT
arm (N = 11,106) and L-DAPT arms (N = 11,112). Our analysis found no
significant difference in the incidence of stroke (RR = 0.95 [0.70-1.29]; p =
0.76), myocardial infarction (RR = 1.15 [0.94-1.4]; p = 0.18), thrombosis (RR =
1.25 [0.86-1.83]; p = 0.25), and all-cause mortality (RR = 0.85 [0.68-1.07]; p
= 0.16) between two arms. However, major bleeding events were less (RR = 0.52
[0.27-1.0]; p = 0.05) in the Abv-DAPT arm than in the L-DAPT arm. Conclusion:
Ticagrelor-based monotherapy after 1 month of ticagrelor-based DAPT could
reduce bleeding complications without compromising ischemic protection.
PROSPERO Registration: (CRD42024536139 - https://www.crd.york.ac.uk/PROSPEROFILES/536139_STRATEGY_20240726.pdf)
Keywords: Dual antiplatelet therapy, ticagrelor, risk of bleeding, stroke,
thrombosis, myocardial infarction, all-cause mortality
Percutaneous coronary intervention (PCI)
is a widely performed procedure for treating coronary artery disease, with its
success rate heavily reliant on the use of dual antiplatelet therapy (DAPT) to
prevent thrombotic complications such as stent thrombosis1. DAPT,
typically consisting of aspirin and a P2Y12 inhibitor, has been the cornerstone
of post-PCI management, particularly in reducing ischemic events during the
critical period following stent implantation. Traditionally, DAPT has been
continued for 12 months or longer, especially in patients at higher risk of
ischemic events2-5. Since prolonged use of DAPT could increase the
risk of bleeding, particularly in patients with a high bleeding risk (HBR) the
optimal duration of DAPT before transitioning to P2Y12 inhibitor monotherapy
remains under active investigation1,3. Balancing the benefits of
ischemic protection against the risks of bleeding is crucial in tailoring DAPT
duration, necessitating strategies that mitigate bleeding risk while
maintaining therapeutic efficacy1,3,4.
Several clinical trials have evaluated the
safety and efficacy of limiting DAPT to 1-3 months, followed by P2Y12 inhibitor
monotherapy in patients who have undergone PCI1,4-6. Notably, trials
such as the MASTER DAPT have demonstrated that abbreviated DAPT regimens can
reduce bleeding complications without increasing ischemic events, suggesting
that this strategy may be particularly beneficial for patients with HBR3.
Furthermore, studies
have indicated that ticagrelor-based monotherapy following a short course of
DAPT, even a 1-month DAPT duration, followed by monotherapy, offers favorable outcomes, including reduced all-cause and cardiovascular mortality1,4.
This meta-analysis
aims to evaluate the safety and efficacy of ticagrelor and aspirin therapy for
1 month or less, followed by ticagrelor monotherapy for 12 months or more
in patients undergoing PCI. By synthesizing data from multiple trials, this
study seeks to clarify whether a shorter DAPT regimen can provide comparable
protection against ischemic events while reducing bleeding risk, thus
potentially offering a safer and more effective treatment strategy for post-PCI
patients.
METHODOLOGY
We aimed to
evaluate the efficacy and safety of ticagrelor monotherapy after abbreviated
exposure (1 month or less) to DAPT composed of ticagrelor and aspirin. We
analyzed data from ULTIMATE-DAPT7, T-PASS8, and
GLOBAL-LEADERS9 trials (Table 1). We systematically searched
PubMed-MEDLINE, EMBASE, Scopus, and the Cochrane Central Registry of Controlled
Trials database to ensure we had caught all the important trials (Fig. 1). Predefined
keywords were short-term Dual antiplatelet therapy OR (“Dual Antiplatelet
Therapy/adverse effects” [MeSH] OR “Dual Antiplatelet Therapy/mortality”
[MeSH]) AND Percutaneous coronary intervention OR Coronary intervention OR
Coronary Revascularization OR
(“Percutaneous Coronary Intervention/adverse effects” [MeSH] OR “Percutaneous
Coronary Intervention/mortality” [MeSH] OR “Percutaneous Coronary Intervention/standards”
[MeSH]) AND Ticagrelor OR P2Y12 inhibitors OR (“Ticagrelor/administration and
dosage” [MeSH] OR “Ticagrelor/adverse effects” [MeSH] OR “Ticagrelor/blood”
[MeSH] OR “Ticagrelor/metabolism” [MeSH] OR “Ticagrelor/pharmacology” [MeSH] OR
“Ticagrelor/therapeutic use” [MeSH]). The detailed search strategy can be found
in the link listed below. No language and publication period restrictions were
applied. Further reference lists of eligible studies, key journals, trial
registers, and internet resources were also searched. Only randomized control
trials were included in the analysis. The current meta-analysis is registered
in PROSPERO (CRD42024536139 - https://www.crd.york.ac.uk/PROSPEROFILES/536139_STRATEGY_20240726.pdf)
|
Table 1. Details of the Studies Included
|
| |
ULTIMATE-DAPT (2024)7
|
T-PASS (2024)8
|
GLOBAL-LEADERS (2018)9
|
|
Study Design
|
Randomized, placebo-controlled, double-blind clinical trial
|
Randomized, multicenter, open-label
|
Randomized, parallel, stratified, concealed
|
|
Key Inclusion Criteria
|
Adults (=18 years of age) who tested positive for NSTEMI or STEMI or
tested negative for unstable angina.
The individual should not have any reported events after their PCI with
DES within 1 month of DAPT.
|
Adults (>18 years) implanted with bioresorbable polymer
sirolimus-eluting stent for ACS.
|
Patients with an implant of a biolimus-eluting stent for ACS and
undergoing PCI.
|
|
Key Exclusion Criteria
|
Patients with a history of stroke (within last 3 months), CABG, or
require a surgery within the 12 months.
|
Individuals with increased bleeding risk, pregnant women or who are
expecting to get pregnant and those with a life expectancy <1 year.
|
Individuals with a contraindication/poor
tolerance to aspirin or ticagrelor, history of use of a CYP3A4 inhibitor,
fibrinolytic therapy (within 24 hours of PCI).
Patients with hepatic disease, history of stroke, risk of bleeding, CABG,
or requiring any other surgery within the next 12 months.
|
|
DAPT Strategy
|
Ticagrelor plus Aspirin
Duration:
Experimental arm: 1 month in (IVUS-ACS) and 1 month from the time of
enrollment
Control arm: 12 months
|
Ticagrelor plus Aspirin
Duration:
Experimental arm: Less than 1 month (Media DAPT duration in the group)
Control arm: 12 months
|
Experimental arm: Aspirin + ticagrelor in the experimental arm (1 month)
Control arm: Aspirin + clopidogrel or ticagrelor for stable or unstable
coronary disease, respectively (12 months).
|
|
Outcome Measures
|
Types of bleeding based on BARC (2, 3, or 5)
Adverse cardiovascular and cerebrovascular events.
|
Bleeding events based on BARC (3 or 5) at 12 months and major adverse
cardiovascular events.
|
All-cause mortality or nonfatal myocardial infarction and bleeding events
based on BARC (3 or 5).
|
|
Median Duration of Follow-up
|
1 Year
|
1 Year
|
2 Years
|
|
Trial Registration
|
NCT03971500
|
NCT03797651
|
NCT01813435
|
NSTEMI = Non-ST-elevated myocardial infarction; STEMI = ST-elevated myocardial infarction; PCI = Percutaneous coronary intervention; DES = Drug-eluting stent; DAPT = Dual antiplatelet therapy; ACS = Acute coronary syndrome; CYP3A4 = Cytochrome P450
3A4; CABG = Coronary artery bypass graft; IVUS = Intravascular ultrasound; BARC = Bleeding Academic Research Consortium.
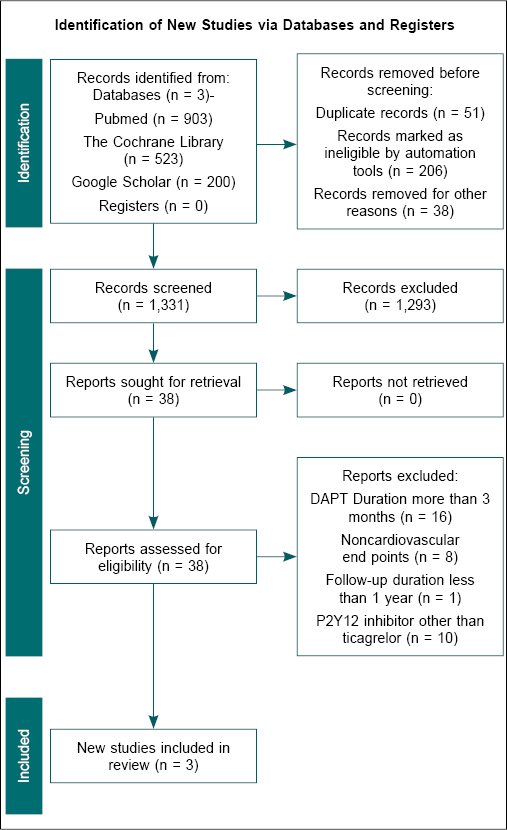
Figure 1. Provides the approach to obtain the studies that fit within the inclusion criteria based on the PICOS strategy.
Inclusion
Criteria
The search included studies with cohorts of
patients who had undergone PCI and had received DAPT with ticagrelor and
aspirin.
Exclusion
Criteria
Studies with a nonrandomized trial design, a
follow-up duration of less than 12 months, and unclear safety and efficacy
points were excluded from the study. Further studies with monotherapy with an
antiplatelet agent other than ticagrelor were also excluded from the study.
Comparator
Groups in the Included Studies
The experimental group consisted of patients who
received DAPT with ticagrelor and aspirin for 1 month or less (Abbreviated
DAPT: Abv-DAPT), followed by ticagrelor monotherapy. In contrast, the control
group included patients who had received DAPT for 12 months or more (Long-term
DAPT: L-DAPT). Both groups had received antiplatelet therapy as part of their
standard post-PCI treatment.
The intervention involved administering DAPT
with ticagrelor (a loading dose of 180 mg,
followed by 90 mg twice daily) plus aspirin (a loading dose of 160-500 mg, followed by 100 mg once daily) for 1 month or less (Abv-DAPT). This was followed by ticagrelor monotherapy (90 mg twice daily) for 12 months or more after the index
PCI.
The comparator was DAPT with any P2Y12 inhibitor
(loading dose followed by the standard daily dose) plus aspirin (loading dose
of 160-500 mg, followed by 100 mg once daily) for 12 months or more
(L-DAPT) after the index PCI.
Similar to the intervention group, antiplatelet
therapy in the control group was part of the standard post-PCI treatment. Table
1 provides the characteristics of the included studies.
Outcome
Measures
The primary outcome was to assess the efficacy
and safety outcomes of interventions. Efficacy outcomes included all-cause
death, cardiovascular death, myocardial infarction, stroke, stent thrombosis,
and urgent target vessel revascularization. Safety outcomes focused on major
and minor bleeding events.
Measures of
Effect
Outcomes for continuous variables were expressed
as mean differences (MD) using conventional units. For studies that report
results in SI units, conversions to conventional units were performed before
analysis. Results were expressed as risk ratios (RR) with 95% confidence
intervals (CI) for dichotomous outcomes, such as treatment success. Absolute
risk differences were calculated for adverse events following treatment. RevMan
Web 5.3 was utilized to compare the MDs of the primary and secondary outcomes
between the Abv-DAPT and L-DAPT groups.
Data
Extraction (Selection and Coding)
Two authors independently extracted data using
standardized forms. If multiple publications from the same study group were
identified, the results were consolidated, and relevant data from each report
was included in the analysis. As mentioned, data on primary and secondary outcomes
was extracted. Patient characteristics, including demographic information and
comorbidities, were documented in a tabular format from the included and
excluded studies. Any disagreements between the authors were resolved by consensus.
Risk of Bias
(Quality) Assessment
Three authors independently assessed the risk of
bias using the Review Manager (RevMan) web software. The evaluation considered
several factors, including adequate sequence generation to avoid selection
bias, proper allocation concealment, and measures to prevent knowledge of
allocated interventions during the study. Additionally, the blinding of
participants, personnel, and outcome assessors was assessed to minimize
performance and detection bias. The assessment ensured that incomplete outcome
data had been appropriately addressed and the study reports were free from
selective outcome reporting. Finally, the study was evaluated for any other
potential sources of bias. A fourth author resolved any disagreements among the
authors.
A random effect model was used for data
analysis, with outcomes expressed as 95% CI. Results were reported as RR with
95% CI for dichotomous outcomes, such as treatment success. Absolute risk
differences were calculated for adverse events post-treatment. Forest plots
were generated using RevMan software, with the left side of the graph favoring
Abv-DAPT and the right side favouring L-DAPT. A p-value of <0.05 was
considered statistically significant.
RESULTS
Our search strategy identified three clinical
trials that compared the efficacy of DAPT consisting of ticagrelor plus aspirin
or clopidogrel plus aspirin for 1 month or less, followed by ticagrelor
monotherapy for 12 months or more in patients undergoing PCI. The total
population for the meta-analysis was 22,218, with a nearly equal distribution
between the experimental (N = 11,106) and control arms (N = 11,112). Baseline
characteristics are as per Table 2. The random-effects model was used to
analyze five critical outcomes: incidence of stroke, major bleeding, myocardial
infarction, stent thrombosis, and all-cause mortality (Fig. 2).
|
Table 2. Baseline Characteristics of Patients
|
|
Parameters
|
ULTIMATE-DAPT7
|
T-PASS8
|
GLOBAL-LEADERS9
|
| |
Abv-DAPT
(n = 1,700)
|
L-DAPT (n = 1,700)
|
Abv-DAPT
(n = 1,426)
|
L-DAPT
(n = 1,424)
|
Abv-DAPT
(n = 7,980)
|
L-DAPT
(n = 7,988)
|
|
Age, years (mean ± SD)
|
62 (21.3%)
|
62.6 (18.9%)
|
61 (10%)
|
61 (10%)
|
64.5 (10.3%)
|
64.6 (10.3%)
|
|
Female (%)
|
436 (25.7%)
|
443 (26.1%)
|
233 (16%)
|
243 (17%)
|
1,865 (23.4%)
|
1,849 (23.1%)
|
|
BMI (kg/m2) mean ± SD
|
-
|
-
|
25.1 (3.6%)
|
25.0 (3.5%)
|
28.2 (4-6)
|
28.2 (4-6)
|
|
Initial presentation
|
|
|
|
|
|
|
|
Stable CAD (%)
|
0
|
0
|
0
|
0
|
4,230 (53.0%)
|
4,251 (53.2%)
|
|
Unstable angina (%)
|
668 (39.3%)
|
708 (41.7%)
|
347 (24%)
|
361 (25%)
|
1,004 (12.6%)
|
1,018 (12.7%)
|
|
NSTEMI (%)
|
545 (32.1%)
|
531 (31.2%)
|
507 (36%)
|
485 (34%)
|
1,684 (21.1%)
|
1,689 (21.1%)
|
|
STEMI (%)
|
487 (28.7%)
|
461 (27.1%)
|
572 (40%)
|
578 (41%)
|
1,062 (13.3%)
|
1,030 (12.9%)
|
|
Medical history
|
|
|
|
|
|
|
|
Diabetes mellitus (%)
|
540 (31.8%)
|
535 (31.5%)
|
422 (30%)
|
408 (29%)
|
2,049 (25.7%)
|
1,989 (24.9%)
|
|
Hypertension (%)
|
1,058 (62.2%)
|
1,063 (62.5%)
|
669 (47%)
|
679 (48%)
|
5,882 (74.0%)
|
5,833 (73.3%)
|
|
Dyslipidemia (%)
|
1,178 (69.3%)
|
1,157 (68.1%)
|
1,048 (74%)
|
1,058 (74%)
|
5,345 (69.3%)
|
5,423 (70.0%)
|
|
Current smoking (%)
|
486 (28.6%)
|
482 (28.4%)
|
557 (39%)
|
537 (38%)
|
2,066 (25.9%)
|
2,103 (26.3%)
|
|
Chronic renal insufficiency (%)
|
119 (7.0%)
|
129 (7.6%)
|
118 (8%)
|
104 (7%)
|
1,099 (13.9%)
|
1,072 (13.5%)
|
|
Previous myocardial infarction (%)
|
143 (8.4%)
|
156 (9.2%)
|
27 (2%)
|
25 (2%)
|
1,831 (23.0%)
|
1,879 (23.6%)
|
|
Previous PCI (%)
|
171 (10.1%)
|
174 (10.2%)
|
92 (7%)
|
92 (7%)
|
2,609 (32.7%)
|
2,612 (32.7%)
|
|
Previous CABG (%)
|
2 (0.1%)
|
4 (0.2%)
|
4 (0.28%)
|
2 (0.14%)
|
448 (5.6%)
|
495 (6.2%)
|
|
Stroke history (%)
|
154 (9.1%)
|
147 (8.7%)
|
43 (3%)
|
49 (3%)
|
210 (2.6%)
|
211 (2.6%)
|
Abv-DAPT = Abbreviated dual antiplatelet therapy; L-DAPT = Long-term dual antiplatelet therapy; SD = Standard deviation; BMI = Body mass index; CAD = Coronary artery disease; NSTEMI = Non-ST-elevated myocardial infarction; STEMI = ST-elevated myocardial
infarction; PCI = Percutaneous coronary intervention; CABG = Coronary artery bypass graft.
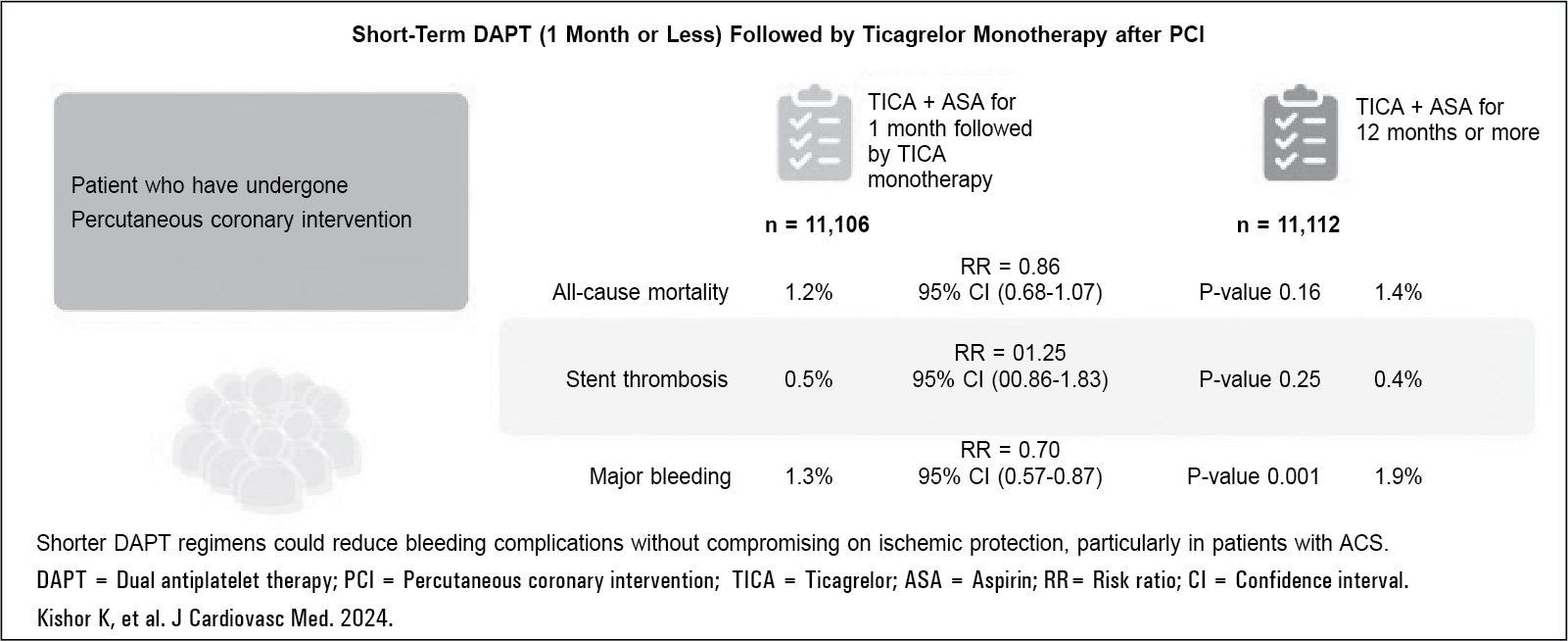
Figure 2. Key finding.
The incidence of stroke was similar between the
control group (n/N = 84/11,112 [0.75%]) and the experimental group (n/N =
80/11,106 [0.7%]). The overall RR was 0.95 (95% CI: 0.70-1.29), with no
significant difference between the groups (p = 0.76).
The risk of major bleeding events was also
comparable between the control group (n/N = 214/11,112 [1.9%]) and the
experimental group (n/N = 145/11,106 [1.3%]). The overall RR for bleeding
events was 0.52 (95% CI: 0.27-1.00), which was not statistically significant (p
= 0.05). Participant characteristics-based subgroup analysis showed higher
bleeding in male patients and those with acute coronary syndrome (ACS).
However, the analysis was limited by significant heterogeneity (Fig. 3).
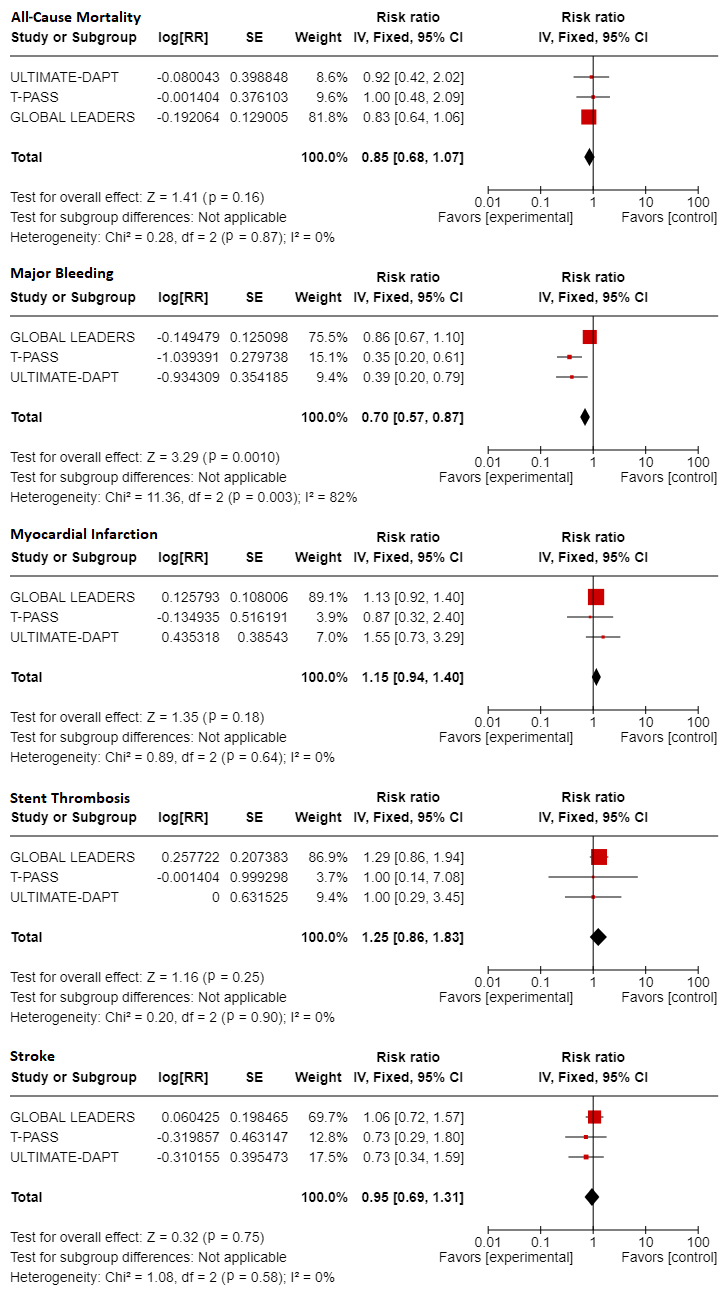
Figure 3. Comparison of the incidence of all-cause mortality, major bleeding, myocardial infarction, stent thrombosis, and stroke between the two groups.
Forrest plots representation of the risk ratio (with 95% CI) of the incidence of all-cause mortality; major bleeding, myocardial infarction, stent thrombosis, and stroke between experimental (Abv-DAPT) vs. control (L-DAPT) groups.
Similarly, the incidence of myocardial
infarction was comparable between the control group (n/N = 277/11,112 [2.5%])
and the experimental group (n/N = 203/11,106 [1.8%]). The overall RR for
myocardial infarction was 1.15 (95% CI: 0.94-1.40), with no significant
difference between the groups (p = 0.18).
The incidence of thrombosis was comparable
between the control group (n/N = 48/11,112 [0.4%]) and the experimental group
(n/N = 60/11,106 [0.5%]). The RR for thrombosis was 1.25 (95% CI: 0.86-1.83),
with no statistically significant differences between the groups (p = 0.25).
The incidence of all-cause mortality was also
similar between the control group (n/N = 158/11,112 [1.4%]) and the
experimental group (n/N = 134/11,106 [1.2%]). The overall RR for all-cause
mortality was 0.85 (95% CI: 0.68-1.07), with no statistically significant
difference between the comparator groups (p = 0.16).
Efficacy outcomes as per age (<65-75 years
and >65-75 years), gender, diabetes, and renal dysfunction subgroups is
shown in Figure 4.
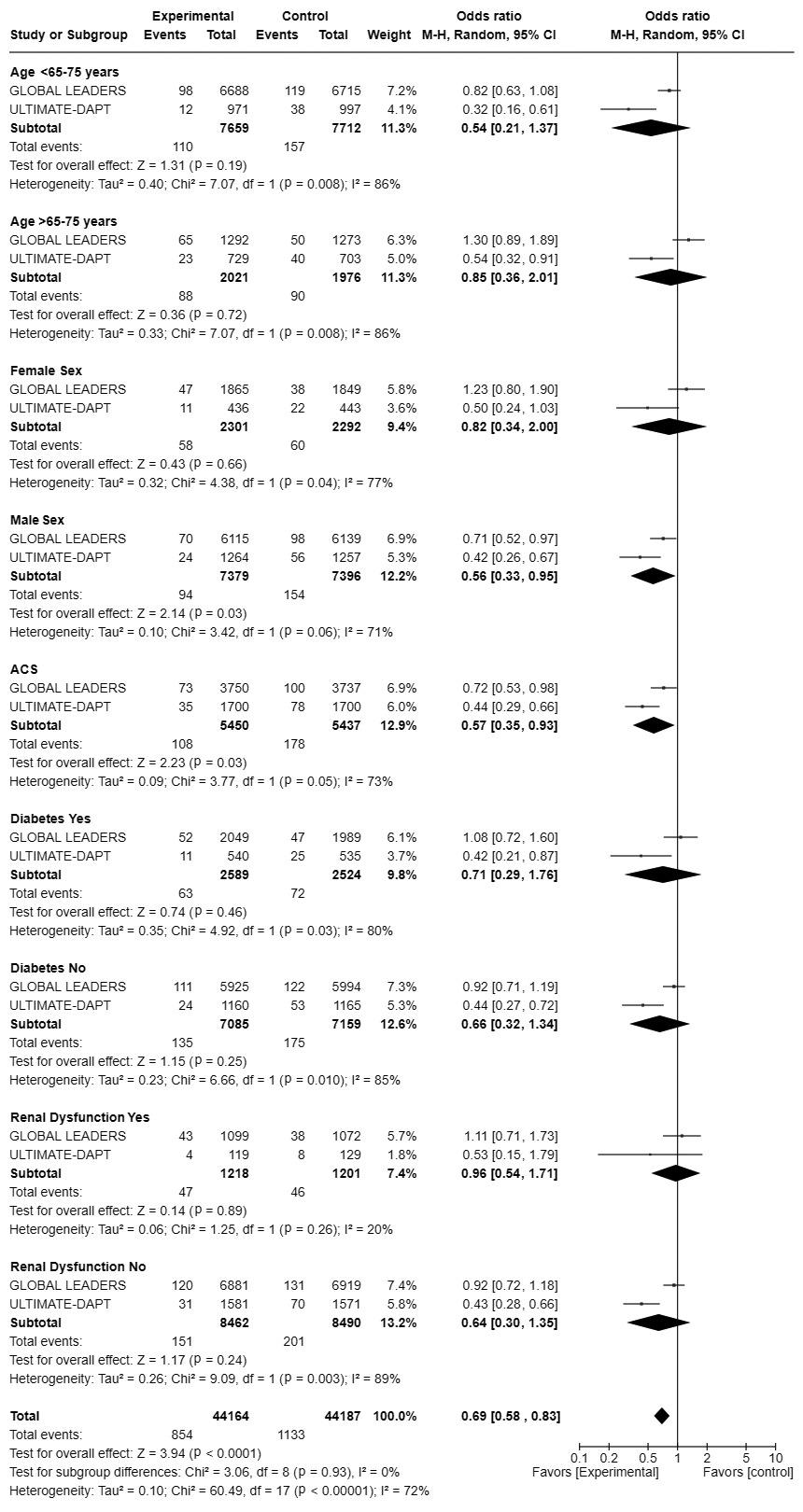
Figure 4. Participant characteristics based subgroup analysis.
Forrest plots representation of the odds ratio (with 95% CI) for the incidence of major bleeding across different participant characteristics between experimental (Abv-DAPT) vs. control (L-DAPT) groups.
DISCUSSION
Dual antiplatelet therapy is a crucial component
of post-PCI care to minimize ischemic events. Considering the benefit-to-risk
ratio, there is a need to optimize the duration of the DAPT regimen to the
shortest yet most effective way of reducing ischemic events, especially in HBR
cohorts. This meta-analysis identified three trials that administered DAPT for
up to 1-month (experimental group) compared to the traditional 12-month period
in the control group. Our results from the meta-analysis found no significant
difference in the incidence of stroke (RR = 0.95 [0.70-1.29]; p = 0.76),
major bleeding events (RR = 0.52 [0.27-1.0]; p = 0.05), incidence of
myocardial infarction (RR = 1.15 [0.94-1.4]; p = 0.18), incidence of
thrombosis (RR = 1.25 [0.86-1.83]; p = 0.25), and incidence of all-cause
mortality (RR = 0.85 [0.68-1.07]; p = 0.16), between the two arms.
The ULTIMATE-DAPT
(2024) randomized, double-blind, placebo-controlled trial consisted of diverse
patient profiles, including those tested biomarker-positive and
biomarker-negative for ACS. The rigorous design of the study and broad
inclusion criteria allowed for a comprehensive assessment of DAPT duration
across different clinical scenarios, ensuring the findings apply to a wide
range of patients7. Similarly, the T-PASS (2024) trial, which focused
on patients with ACS undergoing bioresorbable polymer sirolimus-eluting stent
implantation, provides crucial data on the impact of significantly shortening
DAPT duration. This study compared a median DAPT duration of less than 1 month
with the standard 12-month regimen, assessing a composite outcome of death,
myocardial infarction, thrombosis, stroke, and incidence of any major bleeding
events. A key finding from the T-PASS trial was that stopping aspirin within 1
month and transitioning to ticagrelor monotherapy was noninferior and may be
superior to the 12-month DAPT regimen for the 1-year composite outcome8.
This superiority was reflected by a significant reduction in major bleeding
events, highlighting the potential benefits of a shorter DAPT duration in this
patient population.
Interestingly, the results of the T-PASS trial
contrast with those of the GLOBAL-LEADERS (2018) trial, where a 1-month DAPT
regimen followed by ticagrelor monotherapy did not demonstrate superiority over
the 12-month DAPT regimen in terms of ischemic outcomes8,9. The
primary factor driving the noninferiority in T-PASS was the significantly lower
bleeding rate (1.2% in T-PASS vs. 3.4% in GLOBAL-LEADERS), underscoring the
critical role of bleeding risk in determining the optimal duration of DAPT8.
The findings from ULTIMATE-DAPT and T-PASS are consistent in showing that
ticagrelor monotherapy following a shortened DAPT regimen results in a lower
rate of clinically relevant bleeding while maintaining similar rates of major
adverse cardiovascular and cerebrovascular events compared to more extended
DAPT regimens. Both trials focused on populations with ACS, a group at higher
risk for both ischemic and bleeding complications, making the balancing of
these risks particularly challenging.
Recently, a patient-level meta-analysis
concluded that stopping aspirin 1 to 3 months after PCI followed by ticagrelor
monotherapy is safer and equally effective as standard DAPT4. Unlike
clopidogrel, ticagrelor monotherapy significantly reduced major bleeding events
(53% reduction in major bleeding), while offering comparable protection against
ischemic events10,11. Notably, the use of clopidogrel-based
monotherapy may pose a considerable challenge in patients with high platelet
reactivity12,13. While on clopidogrel-based DAPT, the probability of
ischemic events in such patients increases as soon as the aspirin is
discontinued. The discontinuation of aspirin leaves clopidogrel with suboptimal
platelet inhibition and minimal antiplatelet effect due to high platelet
reactivity. In contrast, ticagrelor offers more consistent and profound P2Y12
receptor inhibition, thereby substantially reducing ischemic events compared to
clopidogrel monotherapy9. The analysis has strengths in combining
patient-level data from three large trials to quantify the risks and benefits
associated with P2Y12 inhibitor monotherapy compared to DAPT continuation after
PCI. It also allows for a detailed assessment of the efficacy and safety of
ticagrelor and clopidogrel monotherapy across different clinical settings.
Additionally, the analysis captures diverse
patient populations and treatment scenarios, enhancing the reliability and
applicability of the findings to routine clinical practice. These results and
the current meta-analysis suggest that an Abv-DAPT duration, especially with
potent P2Y12 inhibitor monotherapy, may effectively balance ischemic risk
without significantly increasing bleeding risk. The evidence supports the
hypothesis that ticagrelor monotherapy could replace aspirin in DAPT regimens,
offering similar protection against ischemic events while reducing the risk of
major bleeding.
However, several critical questions remain
unanswered, such as determining the best molecule for monotherapy to optimally balance ischemic and bleeding risks,
defining the optimal duration of DAPT, and standardizing the factors that should guide DAPT duration in various patient subgroups, such as those who have undergone coronary artery bypass grafting or those at higher risk for bleeding or ischemic events.
The ongoing exploration of these aspects, from
complete aspirin elimination to prolonged DAPT regimens, reflects the
complexity of managing patients’ post-PCI and highlights the need for continued
research to refine DAPT strategies further.
CONCLUSION
In conclusion, this systemic literature review
and meta-analysis contributes valuable evidence to the growing literature
advocating a more personalized approach to DAPT duration. These studies
highlight the potential of shorter DAPT regimens in reducing bleeding
complications without compromising ischemic protection, particularly in
patients with ACS. Future research should address the unresolved issues related
to optimizing DAPT strategies and improve patient outcomes following PCI.
LIMITATIONS
This study has several limitations. First,
although data from three large trials were combined, the overall sample size
may still limit the ability to detect rare safety events and outcomes.
Second, the heterogeneity of the included
trials, such as variations in patient populations, procedural techniques, and
duration of follow-up, may introduce bias and affect the generalizability of
the findings. Additionally, this analysis relies on post-hoc data, which
inherently carries the risk of confounding factors that must be fully accounted
for. The limitation of long-term follow-up hinders the ability to assess the
sustained effects of the intervention strategy.
Acknowledgments: None. No assistance in the preparation of
this article is to be declared.
Artificial
intelligence generated content: Not applicable.
Declarations
Data availability
statement: Not applicable.
Funding statement: None.
Conflict of interest
disclosure: The authors
declare no conflicts of interest.
Patient consent
statement: Not applicable.
Permission to
reproduce material from other sources: Not applicable.
Clinical trial
registration: Not
applicable.
Previous
presentations: None.
Author contributions:Dr Kamal Kishor was
involved in the conception and design, Dr Kamal Kishor, Dr Lakshmi Nagendra, Dr
Devendra Bisht contributed to the analysis and interpretation of the data; Dr
Kamal Kishor, Dr Lakshmi Nagendra drafted the paper; Dr Devendra Bisht and Dr
Kunal Mahajan revised the manuscript critically for intellectual content; and
all authors were involved in approving the final version of the
manuscript. All authors agree to be accountable for all aspects of the work.
REFERENCES
1.
Sardella G, Spirito A, Sartori S, Angiolillo DJ, Vranckx P, Hernandez JMT, et al. 1- versus 3-month DAPT in older patients at a high bleeding risk undergoing PCI: Insights from the XIENCE Short DAPT Global Program. Am J Cardiol. 2024;214:94-104.
2.
Apostolos A, Travlos C, Tsioulos G, Chlorogiannis DD, Karanasos A, Papafaklis M, et al. Duration of dual antiplatelet treatment after percutaneous coronary intervention in patients with diabetes: a systematic review and meta-analysis.
J Cardiovasc Pharmacol. 2024;83(1):64-72.
3.
Landi A, Alasnag M, Heg D, Frigoli E, Malik FTN, Gomez-Blazquez I, et al; MASTER DAPT Investigators. Abbreviated or standard dual antiplatelet therapy by sex in patients at high bleeding risk: a prespecified secondary analysis of a randomized
clinical trial. JAMA Cardiol. 2024;9(1):35-44.
4.
Valgimigli M, Gragnano F, Branca M, Franzone A, da Costa BR, Baber U, et al; Single Versus Dual Antiplatelet Therapy (Sidney-3) Collaboration. Ticagrelor or clopidogrel monotherapy vs dual antiplatelet therapy after percutaneous coronary
intervention: a systematic review and patient-level meta-analysis. JAMA Cardiol. 2024;9(5):437-48.
5.
Tan MC, Dinh D, Gayed D, Liang D, Brennan A, Duffy SJ, et al; Melbourne Interventional Group. Associations between dual antiplatelet therapy score and long-term mortality after percutaneous coronary intervention: analysis of more than
27,000 patients. Can J Cardiol. 2024 Jul 29:S0828-282X(24)00582-8.
6.
Casula M, Casu G, Talanas G, Spano A, Tantry U, Bilotta F, et al. Efficacy and safety of P2Y12 monotherapy vs standard DAPT in patients undergoing percutaneous coronary intervention: meta-analysis of randomized trials. Curr Probl Cardiol.
2024;49(8):102635.
7.
Ge Z, Kan J, Gao X, Raza A, Zhang JJ, Mohydin BS, et al; ULTIMATE-DAPT investigators. Ticagrelor alone versus ticagrelor plus aspirin from month 1 to month 12 after percutaneous coronary intervention in patients with acute coronary syndromes
(ULTIMATE-DAPT): a randomised, placebo-controlled, double-blind clinical trial. Lancet. 2024;403(10439):1866-78.
8.
Hong SJ, Lee SJ, Suh Y, Yun KH, Kang TS, Shin S, et al; T-PASS (Ticagrelor Monotherapy in Patients Treated With New-Generation Drug-Eluting Stents for Acute Coronary Syndrome) Investigators. Stopping aspirin within 1 month after stenting
for ticagrelor monotherapy in acute coronary syndrome: the T-PASS randomized noninferiority trial. Circulation. 2024;149(8):562-73.
9.
Vranckx P, Valgimigli M, Jüni P, Hamm C, Steg PG, Heg D, et al; GLOBAL LEADERS Investigators. Ticagrelor plus aspirin for 1 month, followed by ticagrelor monotherapy for 23 months vs aspirin plus clopidogrel or ticagrelor for 12 months,
followed by aspirin monotherapy for 12 months after implantation of a drug-eluting stent: a multicentre, open-label, randomised superiority trial. Lancet. 2018;392(10151):940-9.
10.
Valgimigli M, Costa F, Lokhnygina Y, Clare RM, Wallentin L, Moliterno DJ, et al. Trade-off of myocardial infarction vs. bleeding types on mortality after acute coronary syndrome: lessons from the Thrombin Receptor Antagonist for Clinical
Event Reduction in Acute Coronary Syndrome (TRACER) randomized trial. Eur Heart J. 2017;38(11):804-10.
11.
Leonardi S, Gragnano F, Carrara G, Gargiulo G, Frigoli E, Vranckx P, et al. Prognostic implications of declining hemoglobin content in patients hospitalized with acute coronary syndromes. J Am Coll Cardiol. 2021;77(4):375-88.
12.
Sibbing D, Aradi D, Alexopoulos D, Ten Berg J, Bhatt DL, Bonello L, et al. Updated expert consensus statement on platelet function and genetic testing for guiding P2Y12 receptor inhibitor treatment in percutaneous coronary intervention.
JACC Cardiovasc Interv. 2019;12(16):1521-37.
13.
Aradi D, Kirtane A, Bonello L, Gurbel PA, Tantry US, Huber K, et al. Bleeding and stent thrombosis on P2Y12-inhibitors: collaborative analysis on the role of platelet reactivity for risk stratification after percutaneous coronary intervention.
Eur Heart J. 2015;36(27):1762-71.