Abstract
Myxomas are the most common primary cardiac tumors, predominantly arising in the left atrium and less frequently in the right atrium or ventricles. Although benign, myxomas can cause significant symptoms and complications due to embolization, obstruction,
or vasoactive substance production. This case report describes a 37-year-old male presenting with intermittent palpitations, anxiety, and breathlessness. Clinical examination and routine investigations were unremarkable except for early finger clubbing.
Echocardiography revealed a pedunculated left atrial mass, later confirmed as a myxoma via histopathological examination. The patient underwent successful surgical resection of the tumor. This case underscores the diagnostic challenges of myxomas,
particularly in asymptomatic individuals, and highlights the importance of echocardiography for detection. Surgical excision remains the definitive treatment, with follow-up to monitor for recurrence. This case report emphasizes the need for awareness
of varied presentations of myxoma and the role of comprehensive cardiac evaluation in symptomatic patients.
Keywords: Asymptomatic cardiac tumor, left atrial myxoma, echocardiography, embolism, surgical resection
Myxomas are the most common primary tumors of the heart and are benign in nature. Seventy-five percent of myxomas arise from the left atrium, either at the mitral valve annulus or the fossa ovalis border of the interatrial septum. Twenty percent arise
from the right atrium, and the remaining 5% may arise from the atria, ventricles, or elsewhere. The familial variety may arise from multiple sites and is often transmitted as autosomal dominant. Myxomas are polyploid, round or oval, gelatinous, with
a white or yellowish-brown color, and with a lobulated or smooth surface. Though mostly benign, recurrence can occur due to inadequate removal. Recurrence is also common with familial myxomas, and distant recurrence has been reported due to embolization1.
Females are more frequently affected than males2.
Symptoms of myxomas could be due to embolization of the tumor, obstruction of valves by the tumor, or vasoactive substances produced by the tumor. Polypoid tumors are more likely to embolize than round ones
3. Embolization can occur in the systemic or pulmonary circulation depending on the tumor’s presence in the left or right atrium, respectively. Embolization to the systemic circulation may cause cerebral, coronary, or peripheral arterial
occlusion, producing relevant symptoms4. Embolization to the pulmonary circulation may cause pulmonary infarction and recurrent embolization pulmonary hypertension. The tumor can obstruct the mitral or tricuspid valves and precipitate sudden
death, most commonly the mitral valve5. Systemic symptoms like fever, arthralgia, weight loss, and Raynaud’s phenomenon may occur, attributed to interleukin-6 (IL-6) produced by the tumor mass. Patients are often asymptomatic and found
to have a cardiac mass when echocardiography is performed for any other purpose.
Physical signs are scanty but signs of left or right heart failure may be observed. Loud and delayed P2 due to pulmonary hypertension, and a systolic murmur due to mitral or tricuspid valve destruction by the tumor may be present. A loud S1 is caused
by a delay in the closure of the mitral or tricuspid valve due to obstruction by the tumor. An early diastolic sound called a tumor plop may be heard. Tumor obstructing the mitral or tricuspid valve may produce a diastolic murmur resembling the murmur
of valvular stenosis. Variability of the diastolic murmur with a change of body posture is said to be pathognomonic of myxoma. In a few cases, clubbing has been observed.
There are no specific laboratory diagnostic tests for atrial myxoma. Normocytic normochromic, microcytic, or hemolytic anemia may be found. Leukocytosis, elevated erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and gamma globulin may be
observed. Serum levels of IL-6 may be raised and can be used as markers of recurrence6.
Two-dimensional echocardiography is good enough for the diagnosis, although transesophageal echocardiography (TEE) is more sensitive. Left atrial myxoma needs to be differentiated from a left atrial thrombus. A thrombus is usually located in the posterior
atrium and has a layered appearance. The presence of a stalk and mobile nature favors left atrial myxoma. Magnetic resonance imaging (MRI) can provide additional information regarding the location of the mass. Preoperative coronary angiography is
valuable in evaluating the vascularity of this tumor7.
Myxomas need to be differentiated from a thrombus, which closely resembles it. Carcinoid heart diseases and valvular heart diseases at times are close contenders. Left atrial myxoma has been wrongly treated as endocarditis8.
Surgery is the treatment of choice, either by median sternotomy or robotically-assisted minithoracotomy9.
CASE REPORT
A 37-year-old male patient presented with a history of intermittent palpitations, anxiety, and breathlessness lasting 5 to 10 minutes, not associated with exertion over the past 3 months. These episodes occurred 4 times during this period. He was employed
as an engineer in Saudi Arabia. He did not report chest pain, fever, body pains, lethargy, or loss of appetite. There was no history suggestive of rheumatic fever during childhood. He had been undergoing annual health checks as mandated for his parents’
employment. While he experienced anxiety about his symptoms, his sleep was not disturbed. He was married with children.
On general examination, he appeared well-built and well-nourished, without anemia or lymphadenopathy. He exhibited early clubbing of the fingers but no cyanosis. No obvious skin abnormalities were noted. Jugular venous pressure was normal and no pedal
or sacral edema was detected. Respiratory examination, normal breath sounds were heard. Cardiovascular examination revealed normal heart sounds with no murmurs detected in sitting and supine positions. Abdominal palpation revealed no hepatosplenomegaly,
and examination of the central nervous system did not reveal any abnormalities.
Laboratory findings showed a total leukocyte count of 11,400 cells/µL, hemoglobin of 15.8 grams %, platelet count of 4,90,000/µL, and ESR of 12 mm/hour. Creatine phosphokinase, lipid profile, liver function tests, and renal functions were within normal
limits. Peripheral smear indicated mild thrombocytosis. Screening tests for hepatitis B surface antigen, hepatitis C virus, and human immunodeficiency virus (HIV) were negative.
Chest X-ray, electrocardiography, and abdominal ultrasound were normal. Echocardiography revealed a pedunculated left atrial mass measuring 2.53 × 1.76 cm suggestive of myxoma (Fig. 1). TEE confirmed this finding. Coronary angiography showed normal
coronary arteries without abnormal tumor circulation.
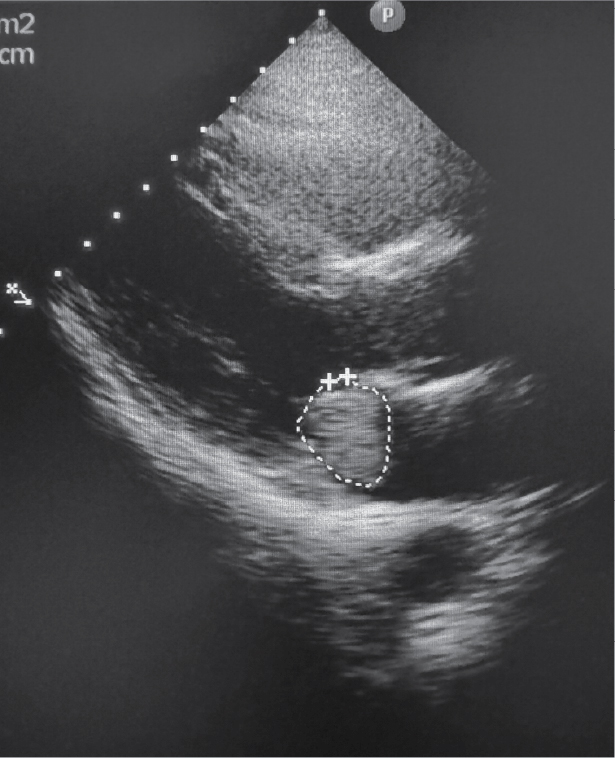
Figure 1. Echocardiography showing a mass of 2.53 × 1.76 cm in the left atrium close to the mitral valve orifice.
The patient underwent surgery, during which the left atrial mass along with the fossa ovalis was excised via a transthoracic approach (Fig. 2). Histopathological examination of the mass revealed stellate, fusiform, and polygonal cells immersed in an amorphous
myxoid matrix consistent with myxoma (Fig. 3). Subsequent monthly reviews postoperatively for 1 year showed no signs of recurrence, and the patient remained asymptomatic.

Figure
2. Specimen of left atrial myxoma along with fossa ovalis, surgically excised.

Figure 3. Histopathological examination of the mass revealed stellate, fusiform, and polygonal cells immersed in an amorphous myxoid matrix consistent with myxoma.
DISCUSSION
Our patient presented with episodic palpitations, breathlessness, and transient anxiety. Left atrial myxomas often present with mild symptoms, posing a diagnostic challenge. Conversely, they can lead to sudden death due to cardiac valve obstruction, commonly
affecting the mitral valve given that 75% of myxomas originate in the left atrium near the mitral valve annulus or fossa ovalis border of interatrial septum, as observed in this case. A subset of cases involves familial myxomas, which typically exhibit
autosomal dominant inheritance and may manifest at multiple cardiac sites.
Symptoms of myxomas vary depending on their effects, whether obstructive, embolic, or through biochemical mechanisms. Our patient did not exhibit systemic symptoms or elevated inflammatory markers suggestive of vasoactive substance secretion by the tumor.
There were no syncopal episodes or signs of flash pulmonary edema indicative of significant valvular obstruction, nor symptoms suggestive of systemic or pulmonary embolism. The tumor measured 2.53 × 1.76 cm, with larger tumors (>5 cm) more likely
to cause valvular obstruction. It had an oval shape; the polypoid shape increases the likelihood of embolization.
No cardiac murmurs were detectable in either sitting or supine positions, nor were there any additional sounds noted. The absence of clinical signs such as a loud and delayed P2 ruled out pulmonary hypertension and pulmonary embolism from the tumor. Clubbing
was the sole clinical sign attributable to the myxoma in our patient, underscoring the diagnostic challenges associated with myxomas.
There are no specific biochemical tests for diagnosing myxomas, although some cases may present with elevated ESR and CRP levels, which were not observed in our case. Reports indicate associations with leukocytosis, anemia, and hemolysis, but our patient
exhibited normal leukocyte counts and had no anemia. Thrombocytopenia has been reported in some cases, whereas our patient had thrombocytosis10.
Echocardiography, performed as part of cardiac screening for symptoms, unexpectedly detected a left atrial mass. It remains the preferred diagnostic modality, with TEE offering higher sensitivity. Cardiac MRI can provide additional details on tumor
location but was unnecessary in our case. Coronary angiography ruled out obstructive coronary artery lesions and vascularization abnormalities of the tumor, revealing normal coronary arteries with no aberrant circulation.
Surgical resection of the tumor, including the fossa ovalis attachment, was performed and sent for histopathological examination. This approach minimizes the risk of recurrence. Postoperative echocardiography confirmed the absence of residual tumor mass
in the left atrium (Fig. 4).
Figure 4. Postoperative Echo showing absence of the tumor in the left atrium.
CONCLUSION
This case highlights the clinical presentation, diagnostic approach, and management of left atrial myxoma in a young male patient. Echocardiography remains pivotal in diagnosis, with surgical excision being curative in most cases. Awareness of familial
predisposition and diligent follow-up are crucial for long-term management.
Acknowledgment
We sincerely thank Dr Sailesh Chalasani, Managing Director, Queen’s NRI Hospital, Visakhapatnam, for allowing us to publish this case.
Declarations
Funding: None.
Conflict of Interest: Non declared.
Ethical approval: Not required.
REFERENCES
1. Larsson S, Lepore V, Kennergren C. Atrial myxomas: results of 25 years’ experience and review of the literature. Surgery. 1989;105(6):695-8.
2. Zheng JJ, Geng XG, Wang HC, Yan Y, Wang HY. Clinical and histopathological analysis of 66 cases with cardiac myxoma. Asian Pac J Cancer Prev. 2013;14(3):1743-6.
3. Ha JW, Kang WC, Chung N, Chang BC, Rim SJ, Kwon JW, et al. Echocardiographic and morphologic characteristics of left atrial myxoma and their relation to systemic embolism. Am J Cardiol. 1999;83(11):1579-82,
4. Lee VH, Connolly HM, Brown RD Jr. Central nervous system manifestations of cardiac myxoma. Arch Neurol. 2007;64(8):1115-20.
5. Rios RE, Burmeister DB, Bean EW. Complications of atrial myxoma. Am J Emerg Med. 2016;34(12):2465.e1-2465.e2.
6. Mendoza CE, Rosado MF, Bernal L. The role of interleukin-6 in cases of cardiac myxoma. Clinical features, immunologic abnormalities, and a possible role in recurrence. Tex Heart Inst J. 2001;28(1):3-7.
7. Hasdemir H, Alper AT, Arslan Y, Erdinler I. Left atrial myxoma with severe neovascularization: role of preoperative coronary angiography. Turk Kardiyol Dern Ars. 2011;39(2):163-5.
8. Kim CH, Je HG, Ju MH, Lee CH. Cardiac myxoma misdiagnosed as infective endocarditis: a case of Carney complex. J Cardiothorac Surg. 2020;15(1):188.
9. Bianchi G, Margaryan R, Kallushi E, Cerillo AG, Farneti PA, Pucci A, et al. Outcomes of video-assisted
minimally invasive cardiac myxoma resection. Heart Lung Circ. 2019;28(2):327-33.
10. Vuopio P, Nikkilä EA. Hemolytic anemia and thrombocytopenia in a case of left atrial myxoma associated with mitral stenosis. Am J Cardiol. 1966;17(4):585-9.