Abstract
Scrub typhus, also called bush typhus, is a zoonotic disease a Gram-negative bacterium. Its presentation may range from nonspecific febrile illness to severe disease, with cardiovascular, renal, hepatic and neurological involvement. Myocarditis is one of the rare complications of scrub typhus. Hence, we are reporting a case of a 50-year-old male, farmer by occupation, presenting to us in multiorgan dysfunction syndrome who developed myocarditis during second week of his illness.
Keywords: Scrub typhus, Orientia tsutsugamushi, myocarditis
Scrub typhus is a zoonotic disease. It is also known as bush typhus or tsutsugamushi disease. It is caused by a Gram-negative bacterium, Orientia tsutsugamushi, which is a member of the Rickettsiaceae family. It is transmitted to humans through the bite of larval mites, known as chiggers. They belong to the family Trombiculidae. While the disease is prevalent worldwide, most of the cases are reported from the so called “tsutsugamushi triangle”, which is a wide area bounded by Pakistan, India and Nepal in the West; Siberia, China, Japan and Korea in the North and Indonesia, Philippines, Australia and the Pacific islands in the South. An estimated 1 million new scrub typhus infections are reported every year and more than 1 billion people globally are at risk. Scrub typhus presentation ranges from mild nonspecific febrile illness to severe disease with cardiovascular, renal, hepatic and neurological involvement. Cardiovascular complications like pericardial effusion, left ventricular systolic dysfunction, diastolic dysfunction, myocarditis and arrhythmias can lead to cardiogenic shock and sudden cardiac arrest. Therefore, the association of scrub typhus-induced cardiovascular disease should be investigated to provide a timely and appropriate diagnosis and to reduce the mortality in complicated scrub typhus infection. Here we are reporting a case of scrub typhus complicated with myocarditis admitted in our hospital.
CASE REPORT
A 50-year-old man with no previous comorbidity was admitted in our hospital with complaints of fever, myalgia and headache since 7 days and nausea/vomiting since 3 days. Upon physical examination, the blood pressure was 130/80 mmHg, pulse rate was 108 bpm, respiratory rate was 18 breaths/min and temperature was 36.8°C. He was alert and fully oriented. Auscultation of both lungs revealed normal vesicular breath sounds and no added sounds. Laboratory testing showed following results: complete blood count – hemoglobin [Hb] - 12.9 g/dL, total leukocyte count [TLC] - 10,680/mm3, platelet count - 75,000/mm3; blood urea – 106 mg/dL; creatinine - 2.21 mg/dL; and liver enzymes – serum glutamic-oxaloacetic transaminase (SGOT) - 219 U/L, serum glutamic-pyruvic transaminase (SGPT) - 182 U/L, alkaline phosphatase - 262 U/L. Chest X-ray was normal and electrocardiograph (ECG) showed sinus tachycardia. Scrub typhus immunoglobulin M (IgM) antibody test was positive (IgM capture enzyme-linked immunosorbent assay [ELISA] test). On Day 4 of admission, patient complained of chest pain and lightheadedness.
On examination, blood pressure was found to be 70/50 mmHg. ECG was suggestive of multiple ventricular premature complexes (Fig. 1). Myocarditis secondary to scrub typhus was suspected. Cardiac enzymes were elevated (Troponin T - 0.86 ng/mL, creatine phosphokinase-MB - 68 ng/mL). Patient was started on inotropes, injection magnesium sulfate and injection hydrocortisone. A two-dimensional echocardiography (2D-Echo) was done which revealed mild mitral and tricuspid regurgitation (Fig. 2 a and b) and global hypokinesia of left ventricle with an ejection fraction (EF) of 25%.
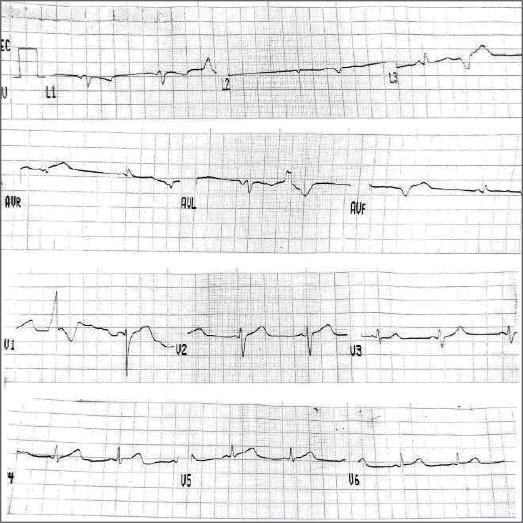
Figure 1. ECG showing multiple premature ventricular complexes with secondary ST-T changes.

Figure 2 a and b. Echocardiographic still images showing mild mitral and tricuspid regurgitation with normal left atrial and ventricular size.
Patient responded well to doxycycline and other supportive care; his condition improved with treatment over the next 48 hours. On Day 6, patient’s blood pressure was 120/80 mmHg. He was slowly weaned off inotropic support. ECG was tracing within normal limits (Fig. 3). Review 2D-Echo was done after 2 weeks which revealed resolution of left ventricular function with EF of 55%. His general condition improved and he was discharged.
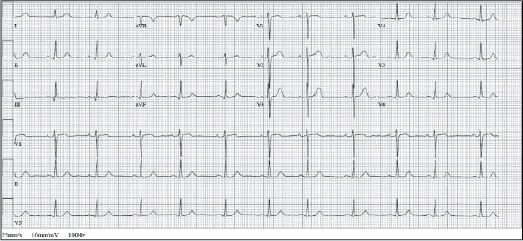
Figure 3. Tracing within normal limits.
DISCUSSION
Scrub typhus is a mite-borne disease predominantly seen in the Asia Pacific region. The typical presentation involves fever, headache, malaise and suffused face. In some cases, especially where early treatment is not instituted, complications may arise, such as meningitis, liver dysfunction, acute kidney injury and disseminated intravascular coagulation, which might lead to multiorgan dysfunction syndrome. The major pathologic findings in tsutsugamushi disease include systemic vasculitis and perivasculitis, which are caused by proliferation of the pathogen in endothelial cells of the microvascular system. These changes are associated within filtration of monocytes, plasma cells and lymphocytes, causing edema or necrosis in the peripheral tissues. Such microangiopathies frequently involve the heart, lungs, brain and kidneys. Various ECG abnormalities including arrhythmias, QRS axis change and ST-T changes have been reported. The heart is one of the target organs of scrub typhus disease. Levine reported that myocardial lesions were observed in around 80% of patients dying from the disease. Vasculitis and perivasculitis in the myocardium induce cellular infiltrations consisting mainly of lymphocytes, monocytes and plasma cells, along with hemorrhage and edema of the interstitial tissues. Cellular infiltrations are also frequently observed in pericardium and endocardium. Myocarditis in scrub typhus is usually subclinical and therefore many times ignored. Tsay and Chang described the serious complications of scrub typhus in 33 patients and only 1 patient (3%) developed myocarditis. A similar study was done by Bhargava et al in a tertiary care hospital in north India, who have described the clinical presentation and predictors of mortality of scrub typhus. Out of a total of 284 patients of scrub typhus, only 2 patients (8.3%) developed myocarditis without acute respiratory distress syndrome or multiorgan failure and both died. Aggarwal et al have reported an incidence of 12% (3 out of 25 cases) for myocarditis in scrub typhus, hence emphasizing further the importance of early recognition of myocarditis.
Until our patient developed hypotension, we did not find any physical warning signs that might have helped us in making an early diagnosis of myocarditis. In our case 2D-Echo showed global hypokinesia of left ventricle with an EF of 25% and helped in making the diagnosis of myocarditis. In ECG, ST abnormalities can be seen in most patients of myocarditis at initial presentation. In our case, ECG revealed ventricular premature complexes. Cardiac biomarkers such as creatine kinase-MB and cardiac troponin-T are noninvasive and highly specific for myocarditis and if available, both can be useful in predicting myocarditis. In our case, both cardiac biomarkers were elevated. Early detection of scrub typhus myocarditis is crucial before patients develop cardiogenic shock and recovery depends on the prompt administration of hemodynamic support and the appropriate antibiotics. The mortality rate is high in severe infection; however, cardiac recovery can be good in those who survive with proper treatment.
Presence of positive serology for scrub typhus, clinical manifestations and abnormal cardiac parameters (cardiac biomarkers and echocardiogram) in our patient were strong evidences for the early diagnosis of myocarditis, which responded very well to the administration of doxycycline and other supportive treatments, resulting in the good cardiac recovery.
CONCLUSION
Myocarditis is a rare cardiovascular complication of scrub typhus. It should always be considered in a patient of scrub typhus with hypotension. The patient should be diagnosed and treated as early as possible to reduce morbidity and mortality. Thus, our case report calls attention to physicians for the possibility of myocarditis in association with scrub typhus.
SUGGESTED READING
- Watt G, Parola P. Scrub typhus and tropical Curr Opin Infect Dis. 2003;16(5):429-36.
- Mahajan SK. Scrub typhus. J Assoc Physicians India. 2005;53:954-8.
- Lee CS, Hwang JH, Lee HB, Kwon KS. Risk factors leading to fatal outcome in scrub typhus patients. Am J Trop Med Hyg. 2009;81(3):484-8.
- Yotsukura M, Aoki N, Fukuzumi N, Ishikawa K. Review of a case of tsutsugamushi disease showing myocarditis and confirmation of Rickettsia by endomyocardial biopsy. Jpn Circ J. 1991;55(2):149-53.
- Levine HD. Pathologic study of thirty-one cases of scrub typhus fever with especial reference to the cardiovascular system. Am Heart J. 1946;31:314-28.
- Fang CY, Dennis DT, Lee JB. Electrocardiographic changes in scrub typhus patients. Southeast Asian J Trop Med Public Health. 1977;8(4):503-9.
- Allen AC, Spitz A comparative study of the pathology of scrub typhus (Tsutsugamushi disease) and other Rickettsial diseases. Am J Pathol. 1945;21(4):603-81.
- Tsay RW, Chang FY. Serious complications in scrub J Microbiol Immunol Infect. 1998;31(4):240-4.
- Bhargava A, Kaushik R, Kaushik RM, Sharma A, Ahmad S, Dhar M, et al. Scrub typhus in Uttarakhand & adjoining Uttar Pradesh: Seasonality, clinical presentations & predictors of mortality. Indian J Med Res. 2016;144(6):901-9.
- Aggarwal HK, Jain D, Kaverappa V, Mittal A, Yadav S, Gupta A. Emergence of scrub typhus in northern India: experience from tertiary care Klimik Dergisi. 2014;27(1):6-11.
- Peter JV, Sudarsan TI, Prakash JA, Varghese GM. Severe scrub typhus infection: Clinical features, diagnostic challenges and management. World J Crit Care Med. 2015;4(3):244-50.