Abstract
Chronic
kidney disease (CKD) and hypertension can lead to each other. Majority of the
patients with CKD have hypertension. Sympathetic overactivity has been
suggested as one of the important etiologies of hypertension in CKD patients.
Clonidine is used as a central sympatholytic to control hypertension in CKD
patients. Drug-induced sialadenitis has been reported with multiple drugs
including antihypertensives. We report a case of clonidine-induced
sialadenitis, which has been rarely seen despite the widespread use of this
drug among CKD patients requiring multiple antihypertensive drugs.
Keywords: Hypertension, clonidine,
sialadenitis, parotitis
Chronic
kidney disease (CKD) currently affects more than 10% of the world population1.Majority of the CKD patients have hypertension, which is considered one of the leading causes
of increased cardiovascular disease (CVD) among CKD population2.
Usually CKD patients with hypertension require multiple antihypertensive drugs
for optimization of blood pressure (BP)3. Clonidine is one of those
extensively used antihypertensives with central
sympatholytic effect4. Parotitis has been reported with other
antihypertensives like nicardipine, nifedipine, captopril, and ramipril, but despite animal studies showing effect on
salivation its very rare to find parotitis with clonidine5. We are reporting here in a rare case of clonidine-induced bilateral parotitis. To the best of our knowledge,
this is the first reported case of bilateral parotitis caused by clonidine.
CASE REPORT
A 58-year-old gentleman presented to the
Emergency Room of our hospital with generalized weakness and sweating for about
an hour. He denied any history of chest pain, retrosternal heaviness,
breathlessness, headache, vomiting, weakness of any limb or similar such
episode in the past. He denied any history of fever and he did not have any
urinary complaints. He had a history of diabetes mellitus and hypertension
since 1 year and was taking tablet glimepiride 2 mg and tablet amlodipine
5 mg post-breakfast daily. He denied any other chronic illness, drug allergy or
any atopic history. He was a nonalcoholic and nonsmoker.
On examination, his pulse was 84/min and his BP
was 160/100 mmHg with SpO2 of 97% on room air. He had pallor and his
systemic examination was within normal limits. His blood glucose was 55 mg/dL.
His electrocardiogram (ECG) showed normal sinus rhythm and arterial
blood gas showed mild metabolic acidosis with calculated bicarbonate of 21
mEq/L. He was promptly managed with intravenous dextrose and tablet amlodipine
was increased to 10 mg/day with which he improved symptomatically with normal
blood sugar and BP levels.
He underwent further evaluation, which showed
hemoglobin 10.0 g/dL, serum creatinine 2.4 mg/dL, serum potassium 5.5 mEq/L,
serum calcium 8.2 mg/dL, and inorganic phosphorus 6.0 mg/dL. Urine, dipstick
showed albumin 2+ and ultrasonography showed normal sized kidneys. Funduscopy
showed mild nonproliferative diabetic retinopathy in both eyes. Once he was
admitted he was not on any oral hypoglycemic agent and on monitoring, his blood
sugar levels were within normal limits.
His BP was controlled with tablet amlodipine 10
mg in the morning.
On the second day of his admission, he
complained of headache without any other associated symptoms. His BP was
160/100 mmHg in the evening with blood glucose of 110 mg/dL and hence the
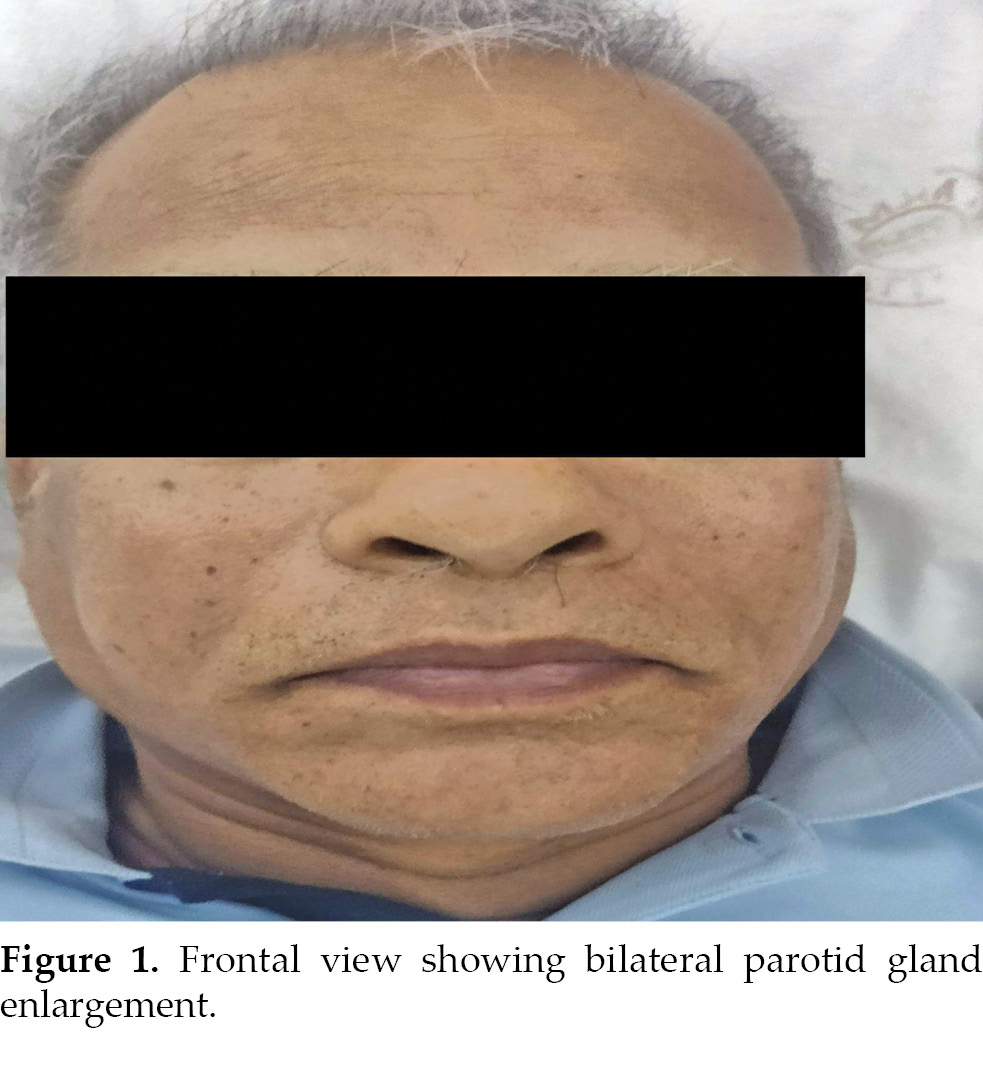
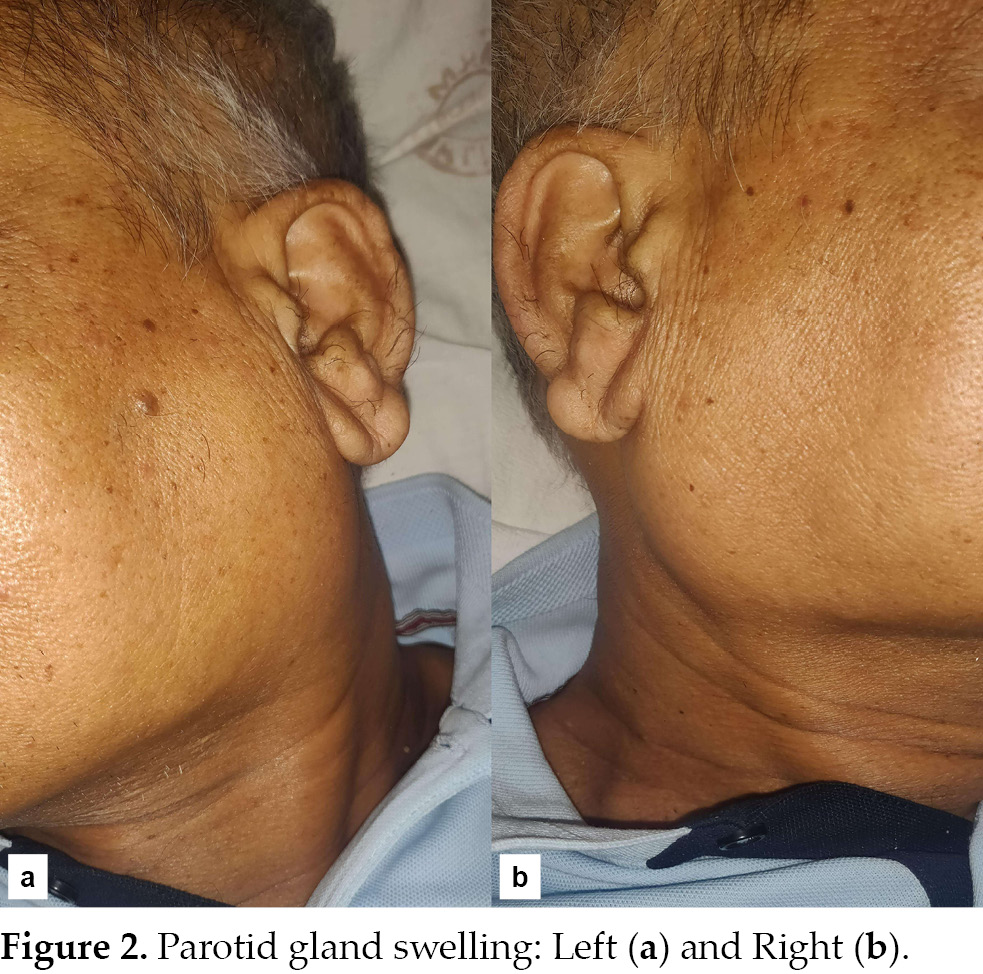
resident on call gave him tablet clonidine 100 µg. He developed bilateral
parotid swelling in about 20 to 30 minutes after taking clonidine. There were
no symptoms suggestive of angioedema such as wheezing, swelling of other
mucosal or submucosal tissues, rash or pruritus. He denied history of dry mouth
or excessive salivation, pain in the swelling, difficulty in swallowing. His
vitals were normal and systemic examination was within normal limits. He had
bilateral painless parotid enlargement (Figs. 1 and 2). He was given oral
antihistaminics and the swelling decreased over the next few hours and
over the next 2 to 3 days it totally disappeared. Even on follow-up patient was
asymptomatic and on examination, he did not have parotid swelling. He was
continued on tablet amlodipine 10 mg OD with blood glucose and BP monitoring.
DISCUSSION
Hypertension affects~30% of the general adult
population and up to 90% of those with CKD6. It is both a cause and
effect of CKD and both are independent risk factors for CVD and lowering BP can
slow glomerular filtration rate (GFR) decline as well as reduce cardiovascular
events7.
There are different mechanisms contributing to
the development of hypertension in CKD and hence influencing its management
like increase in sympathetic tone brought about by afferent signals generated
by functionally declining kidneys, renin-angiotensin-aldosterone system
activation, which promotes salt and water retention, endothelial dysfunction in
advanced CKD (eGFR <30 mL/min/1.73 m2) and increased arterial
stiffness throughout the spectrum of CKD8.There is a
limited evidence on the use of specific antihypertensive agents to treat high
BP in CKD and majority will need combinations of two or more antihypertensive
drugs for achieving the BP goals3.Any antihypertensive
treatment algorithm in CKD, beyond monotherapy, is based on expert opinion,
pathophysiologic or pharmacodynamic considerations, patient tolerance, patient
preferences, comorbid illnesses, etc. The treatment algorithm for intensive systolic
BP arm in SPRINT (Systolic Blood Pressure Intervention Trial) protocol
suggested to begin with 2- or 3-drug therapy using a combination of a
thiazide-type diuretic, and/or an angiotensin-converting enzyme (ACE) inhibitor
or angiotensin receptor blocker but not both and/or a calcium channel blocker
(CCB)9.
Clonidine or
2-(2,6-dichlorophenylamino)-2-imidazoline hydrochloride is a 40-year-old
imidazoline derivative that acts centrally on pre-synaptic alfa-2 receptors
located in the rostral ventrolateral medulla. It reduces the sympathetic
outflow from the central nervous system and decreases plasma norepinephrine
levels leading to decreased cardiac output and reduction in BP10.It is commonly used in CKD patients because of the hypertension pathology
in CKD as explained earlier and requirement of multiple antihypertensive drugs
in CKD patients for optimal BP control.
Parotitis is described as the swelling and
inflammation of one or both parotid glands. Unilateral parotitis is usually
associated with ductal obstruction, whereas bilateral parotitis more likely
reflects systemic causes with common
etiologies like viral and bacterial infections, ductal obstruction and systemic noninfectious causes such as Sjogren syndrome5.Drug-induced parotitis, while rare, has been reported with numerous drugs like l-asparaginase, clozapine,
phenylbutazone, methyldopa, interferon-alfa, oxyphenbutazone, trimethoprim/sulfamethoxazole, chlormethiazole, methimazole, naproxen, nitrofurantoin, sulfadiazine, cytarabine, cimetidine, ranitidine, and thioridazine
5.Among antihypertensives, nicardipine, nifedipine, ramipril, and captopril have been reported to cause parotitis11. No reports were found that implicated other CCBs in the development of parotitis, so it should not be considered
a class effect.
In our case with the temporality of events and
the scarcity of drugs patient was being treated with, clonidine was highly
likely to have caused this rare adverse event and the Naranjo Adverse Drug
Reaction Probability Scale12 showed probable adverse drug reaction
for the clonidine-induced parotitis in our case. The other important learning
was to rule out the dreaded anaphylactic reaction associated with ACE
inhibitor, which patient might be taking for hypertension and can lead to
catastrophic event if not dealt promptly, which fortunately our patient did not
have.
CONCLUSION
Hypertension affects majority of patients
suffering with CKD. Blood pressure control reducescardiovascular morbidity,
mortality, and slows the decline of GFR. Patients with CKD require multiple
drugs for BP control and clonidine is one of the commonly used drugs in this
cohort of patients. Acute parotitis has been associated with few antihypertensive
drugs and can cause panic for the patient and the treating physician. Our
patient had this rare side effect and that too with clonidine, which has very
rarely been seen and can be managed easily with prompt diagnosis and
appropriate intervention.
REFERENCES
1. Kovesdy CP. Epidemiology of chronic kidney disease: an update 2022. Kidney Int Suppl (2011). 2022;12(1):7-11.
2. Collins AJ, Foley RN, Chavers B, Gilbertson D, Herzog C, Ishani A, et al. US Renal Data System 2013 Annual Data Report. Am J Kidney Dis. 2014;63(1 Suppl):A7.
3. Kidney Disease: Improving Global Outcomes (KDIGO) Blood Pressure Work Group. KDIGO 2021clinical practice guideline for the management of blood pressure in chronic kidney disease. Kidney Int. 2021;99(3S):S1-S87.
4. Kuzmin OB, Buchneva NN, Zhezha VV, Serdyuk SV. Uncontrolled arterial hypertension: kidney, neurohormonal imbalance, and approaches to antihypertensive drug therapy. Kardiologiia. 2019;59(12):64-71.
5. Brooks KG, Thompson DF. A review and assessment of drug-induced parotitis. Ann Pharmacother. 2012;46(12):1688-99.
6. Muntner P, Anderson A, Charleston J, Chen Z, Ford V, Makos G, et al; Chronic Renal Insufficiency Cohort (CRIC) Study Investigators. Hypertension awareness, treatment, and control in adults with CKD: results from the Chronic Renal Insufficiency
Cohort (CRIC) Study. Am J Kidney Dis. 2010;55(3):441-51.
7. Gansevoort RT, Correa-Rotter R, Hemmelgarn BR, Jafar TH, Heerspink HJ, Mann JF, et al. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet. 2013;382(9889):339-52.
8. Pugh D, Gallacher PJ, Dhaun N. Management of hypertension in chronic kidney disease. Drugs. 2019;79(4):365-79.
9. SPRINT Research Group; Wright JT Jr, Williamson JD, Whelton PK, Snyder JK, Sink KM, Rocco MV, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373(22):2103-16.
10. Yasaei R, Saadabadi A. Clonidine. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459124/
11. Chauhan V, Negi RC, Sharma A, Gupta S, Mokta J, Verma B, et al. Enalaprilat induced acute parotitis. J Assoc Physicians India. 2008;56:128-9.
12. Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239-45.